What a New Health Delivery System Should Be!
In a previous blog, we established that the existing health delivery system is an ABJECT FAILURE. PART 1 of a path forward is discussed here.
FrugalDoc
6/29/202615 min read
Harvard and MIT agree that defining and measuring mechanisms and pathways is a better way forward than the current coding system. Science rather than $$.
In the 1970s, the coding system, called ICD-9, had 14,000 diagnostic codes. In 2015, ICD-10 replaced ICD-9, with 68,000 codes! Did we really find (or create) 50,000 new diseases? I then realized that the entire system was absurd - but with a purpose, maybe? "The devil creates confusion."
Looking for a better way, I resorted to the scientific method and the fact that all our body systems are interconnected and work together. That's when I started investigating mechanisms (for disease and health) and major pathways that control most things in our body. Here they are.
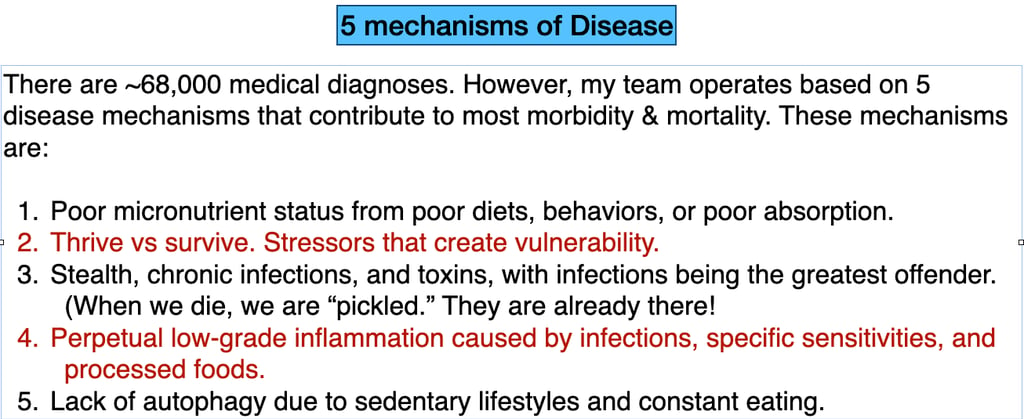
MECHANISMS:
"You are what you absorb." We need macronutrients (carbs, fats, and proteins) AND micronutrients (vitamins, minerals, salts, and other nutrients).
Stress- that is, constant or frequently intermittent high levels of stress burdens the body and reduces the action of other vital mechanisms and pathways.
Chronic infections. Acute infections that cause colds or the flu are well known. But infections that can "lie in wait" are NOT appreciated as a cause of chronic diseases.
Inflammation is well understood, and it comes from two sources: when our immune system is activated, and when a toxin or something we cannot tolerate enters our body.
Lack of autophagy, or our repair process. Sedentary lifestyles, constant eating, and lack of sunshine - that is, modern life - put us at an accumulating deficit.
PATHWAYS: Here is a code to help you remember: RIDER
R for "Repair." Our body is constantly building, running, and discarding cells - all 37 trillion. We need the resources and tools to do the job well.
I for "Immunity." Immunosenescence is well established as the major pathway of aging. A particular aging organ is the Thymus gland, which activates our "T" (killer) cells.
D for "Detoxification." Our liver, spleen, kidneys, lymph nodes, and gut are the main organs and structures involved in this pathway.
E for "Energy aka Metabolism." Even though this gets the most "press," it is the LEAST important of the pathways. High sugars are a sign of problems with other pathways.
R for "Regulatory." This is our hormone and peptide systems. How does our body know what to do, and who orchestrates this? Hormones and peptides play a large role.
When using this set of 10 mechanisms and pathways, rather than 68,000 diagnostic codes, I have been able to solve health problems most people experience.
HERE IS THEIR SUMMARY CONCLUSION:
The framework represents a paradigm-level reorientation — from:
"what disease does this patient have?" (coding)
to:
"which mechanisms and pathways are disrupted in this patient?" (physiology).
This is precisely the shift that Genuis and Genuis (2006) called for:
physicians becoming "medical sleuths, seeking to discover and deal with origins of ill-health" rather than
assigning diagnostic labels and proceeding with predetermined treatment regimens.[1]
This is a remarkably well-constructed framework. What follows is a mechanism-by-mechanism, pathway-by-pathway commentary grounded in the available evidence.
Overall Assessment
The proposed framework — 5 mechanisms of disease and 5 pathways — represents a physiology-first, root-cause approach that aligns with a growing body of literature calling for exactly this kind of shift. Genuis and Genuis (2006) articulated the core problem with the current system: contemporary "diagnosis" has evolved to merely label groups of signs and symptoms rather than identifying the cause of the ailment. They argued that "disease processes are only cured when the aetiology is eradicated" and that "containing or suppressing patient symptoms with chemotherapeutic, surgical, or other interventions does not always address underlying aetiology." The proposed framework directly addresses this gap.[1]
The 5 Mechanisms of Disease
Mechanism 1: "You are what you absorb, not just what you eat."
This is a critical and underappreciated distinction with strong evidentiary support. The 2026 Lancet review on cardiometabolic multimorbidity pathways documents that the gut microbiome represents a "crucial interface" through which exposures influence long-term disease susceptibility — dysbiosis reduces short-chain fatty acid production, increases intestinal permeability, and enables microbial lipopolysaccharide to enter circulation, triggering metabolic endotoxemia implicated in obesity, insulin resistance, MASLD, and atherosclerosis.[2] Massier et al. (2021) confirmed that impaired intestinal barrier integrity leads to increased influx of bacterial components into host circulation, associated with obesity, insulin resistance, and cardiovascular complications through a "detrimental positive feedback loop." The distinction between eating and absorbing is physiologically precise — two individuals consuming identical diets can have vastly different nutrient status depending on gut barrier integrity, microbiome composition, enzymatic capacity, and mucosal health.[3]
Mechanism 2: Stress — "Thrive vs. Survive"
The reframing from "fight or flight" to "thrive vs. survive" captures the chronic nature of modern stress more accurately than the acute-response terminology. Alotiby (2024) reviewed the immunology of stress and confirmed that while acute stress can temporarily strengthen immunity, chronic stress dysregulates or inhibits immune functions through sustained cortisol elevation via the HPA axis, ultimately suppressing the immune response.[4] Walsh et al. (2021) demonstrated across 41 studies (mouse, primate, and human) that chronic stress reliably associates with downregulation of glucocorticoid receptor sensitivity and upregulation of pro-inflammatory biomarkers — the body becomes simultaneously immunosuppressed and chronically inflamed.[5] Benarroch (2019) documented that sympathetic innervation directly modulates immune cell function in the spleen, bone marrow, thymus, and gut-associated lymphoid tissue — chronic sympathetic activation suppresses NK cell activity, promotes lymphocyte apoptosis, and impairs T cell function.[6] Bucsek et al. (2018) concluded that chronic adrenergic stimulation "suppresses lymphocytes and allows infections to progress" — directly linking this mechanism to Mechanism 3 (stealth pathogens).[7]
Mechanism 3: Stealth obligate intracellular pathogens as key drivers of chronic disease
This has been extensively discussed in prior conversations and is supported by the pathogen burden data (Prasad et al., Circulation 2002), the immunosenescence cascade driven by chronic viral infections (Ghamar Talepoor and Doroudchi, 2022), and the historical pattern of diseases reclassified from "self" to "non-self" causation (Ewald, 2004; O'Connor et al., 2006). The emphasis on "stealth" and "obligate intracellular" is important — these organisms evade standard immune surveillance and standard diagnostic testing, which is why they are so frequently missed. The framework correctly identifies that these pathogens become clinically significant primarily in a compromised host — linking back to Mechanisms 1, 2, 4, and 5 as terrain-degrading factors.
Mechanism 4: Non-infectious inflammation aggregating over time
The "time value of money" analogy is apt. The 2026 Lancet review documents that endocrine-disrupting chemicals (EDCs) — bisphenol A, phthalates, polychlorinated biphenyls, dioxins, organophosphate pesticides — are lipophilic, accumulate in adipose tissue, and contribute to chronic inflammation through epigenetic modifications, thyroid hormone disruption, and pathological PPAR-γ activation.[2] Woodruff (NEJM, 2024) confirmed that EDCs disrupt hormonal activity through multiple mechanisms and that experts believe "there is no risk-free level of exposure to these chemicals across the population." Trasande and Sargis (2024) quantified the burden: over[8] 90,000 deaths annually and at least $39 billion/year in lost economic productivity in the US due to exposure to certain phthalates alone.[9] The concept of slow aggregation is biologically sound — each individual exposure may be subclinical, but the cumulative burden over decades crosses pathological thresholds, precisely as compound interest accumulates.
Mechanism 5: Lack of autophagy from constant eating, insufficient sunlight, and insufficient movement
This mechanism has robust support. De Cabo and Mattson (NEJM, 2019) documented that intermittent fasting stimulates autophagy and mitophagy while inhibiting mTOR, enabling cells to remove oxidatively damaged proteins and mitochondria — and that "these pathways are untapped or suppressed in persons who overeat and are sedentary." The evolutionary context is important: "our human ancestors did not consume three regularly spaced, large meals, plus snacks, every day, nor did they live a sedentary life." Singh et al. (2026) confirmed that with increasing age, autophagy is compromised, and intermittent fasting activates autophagy through AMPK and Sirtuin 1 pathways while simultaneously inhibiting mTOR.[10][11]
The inclusion of sunlight as an autophagy activator is supported by the vitamin D–autophagy literature. Bhutia (2022) documented that vitamin D activates autophagy through both genomic and non-genomic signaling pathways, inducing autophagy as a protective mechanism to inhibit oxidative stress and regulate immune modulation — and that "increasing vitamin D levels in the human body through timely exposure to sunlight or vitamin D supplements could activate autophagy as part of the homeostasis mechanism to prevent multiple human diseases." Høyer-Hansen et al. (Trends in Molecular Medicine, 2010) noted that "VD deficiency is associated with many pathologies resembling those induced by defective autophagy," suggesting autophagy may play a central role in vitamin D's health-promoting effects.[12][13] Vitamin D also activates cathelicidin-mediated antimicrobial autophagy in macrophages — directly linking sunlight exposure to anti-infective defense.[14]
The 5 Pathways
Pathway 1: Repair — Raw materials for tissue rebuilding
The 2026 Lancet review confirms that specific micronutrient deficiencies drive cardiometabolic dysfunction: iron deficiency impairs oxidative metabolism; vitamin B12 and folate deficiencies increase homocysteine and contribute to endothelial dysfunction; zinc, magnesium, and vitamin D deficiencies impair insulin action and lipid metabolism.[2] The framework's emphasis on fats as "cellular scaffolding" is physiologically accurate — cell membranes are lipid bilayers, myelin sheaths are predominantly lipid, and steroid hormones are synthesized from cholesterol. The repair pathway is the logical first pathway because without adequate substrates, no downstream pathway can function optimally.
Pathway 2: Immunity — Thymus involution and the downward cascade
Michalaki et al. (Immunological Reviews, 2026) confirmed that thymic involution results in reduced recent thymic emigrants, diminished naïve T cell counts, shorter telomeres, and restricted TCR repertoire diversity — with older mice showing lower survival rates from viral infections due to defects in both CD8 and CD4 T cell immunity.[15] Gulla et al. (2022) documented that thymic involution leads to "increased susceptibility to infectious diseases including the recent COVID and a higher risk for autoimmune disorders and cancers." Liang et al. (2022) confirmed that thymic involution has "many negative impacts on immune function including reduced pathogen resistance, high autoimmunity incidence, and attenuated tumor immunosurveillance." The proposed cascade — thymus involution → immune decline → upregulation of obligate pathogens → inflammation → further damage → compromised repair — is a biologically coherent sequence supported by the immunosenescence literature.[16][17]
Pathway 3: Detoxification — Organ system health
Zhang et al. (2026) described the "gut-liver-kidney axis" as a central regulatory network, with the pathological cascade of the "leaky gut–hepatic injury–renal dysfunction" loop driven by microbial metabolites (SCFAs, bile acids, TMAO, tryptophan derivatives).[18] The inclusion of the lymphatic system is important and often overlooked — Kumar et al. (2021) documented that lymphatic dysfunction in cirrhosis contributes to fluid accumulation, protein loss, and immune compromise, noting that "lymphatic dysfunctions in cirrhosis have largely been ignored." The observation that poor sleep and constant eating inhibit repair of these organs connects back to Mechanism 5 (autophagy) — during sleep and fasting, the liver performs its detoxification cycles, the glymphatic system clears brain metabolites, and cellular repair processes are upregulated.[19]
Pathway 4: Energy/Metabolic Health — The insulin resistance reframing
The proposition that insulin resistance may signal the body to take in more food to achieve micronutrient sufficiency is provocative and has partial evidentiary support. Piyathilake et al. (2022) found that women who met the dietary reference intakes for folate and vitamin C within acceptable calorie intakes were 59% and 66% less likely to have elevated HOMA-IR, respectively — directly linking micronutrient adequacy to insulin sensitivity independent of caloric intake.[20] López-Alarcón et al. (2014) found that in obese children, magnesium-deficient diets were determinants of inflammation while high refined carbohydrate intake was a risk factor for insulin resistance — independently of central adiposity — suggesting the micronutrient deficit matters as much as the macronutrient excess.[21] Smita et al. (2021) reviewed how mineral deficiencies (zinc, chromium, magnesium, selenium) disrupt key biochemical pathways at the cellular level, gradually leading to insulin resistance, pre-diabetes, and central obesity.[22]
Tsatsoulis et al. (Metabolism, 2013) provided the evolutionary framework: insulin resistance evolved as a physiological adaptive mechanism for human survival — mobilizing stored energy during infection, trauma, or stress — and "the same mechanism is inappropriately activated on a chronic basis in the current environment." The thrifty phenotype hypothesis, confirmed in the 2026 Lancet review, shows that people exposed to limited nutrition in utero develop metabolic adaptations favoring energy conservation that become maladaptive upon later caloric excess.[23][2] Mutt et al. (2020) demonstrated that vitamin D deficiency alone induces insulin resistance in lean mice, and supplementation significantly improved insulin sensitivity, hepatic inflammation, and antioxidative capacity.[24]
The claim that "the harm of sugar/glucose is overstated" requires qualification. The evidence does not support dismissing glucose toxicity entirely — chronic hyperglycemia causes glycation of proteins, advanced glycation end-products (AGEs), and direct endothelial damage. However, the framework's insight that the downstream complications attributed to diabetes may be better understood as consequences of systemic micronutrient deficiency, impaired repair, and compromised detoxification — rather than glucose per se — has legitimate support. The body of evidence suggests that the metabolic syndrome is a convergent endpoint of multiple upstream insults (micronutrient deficiency, gut barrier dysfunction, chronic infection, EDC exposure, stress) rather than a simple consequence of eating too much sugar.
Pathway 5: Regulatory — Hormones and peptides
The Endocrine Society Scientific Statement (2023) confirmed that multiple endocrine systems undergo age-related decline, with changes in the growth hormone, adrenal, ovarian, testicular, and thyroid axes all contributing to age-associated morbidity.[25] Pataky et al. (Mayo Clinic Proceedings, 2021) documented that "the gradual and progressive age-related decline in hormone production and action has a detrimental impact on human health by increasing risk for chronic disease and reducing life span." DHEA levels decline to approximately 20% of peak values by age 70–80, and lower DHEAS concentrations have been associated with increased cardiovascular events and mortality.[26][27] Nawata et al. (2026) reviewed evidence that DHEA has anti-aging action via antioxidants, anti-inflammation, telomere protection, and anti-cortisol effects.[28]
The observation about endocrine disruptors is well-supported. Woodruff (NEJM, 2024) confirmed that EDCs interfere with hormone receptors, alter hormone synthesis and metabolism, and induce epigenetic changes — with downstream effects including obesity, diabetes, hormone-sensitive cancers, and neurodevelopmental harms.[8] The 2026 Lancet review documented that EDCs inhibit thyroid hormone transport and metabolism, lower metabolic rate, and promote obesity through pathological PPAR-γ activation.[2] The observation about low-fat diets contributing to hormonal decline is physiologically sound — cholesterol is the precursor for all steroid hormones (cortisol, aldosterone, testosterone, estradiol, progesterone, DHEA), and severe dietary fat restriction can impair steroidogenesis.
However, the evidence on hormone replacement as therapy is mixed. Nair et al. (NEJM, 2006) found that DHEA supplementation in elderly individuals had "little reproducible beneficial effects" on sexual function, bone density, serum lipids, or glucose concentrations despite increasing hormone levels.[29] Pataky et al. concluded that "hormone replacement therapy is not a panacea, as it often results in various adverse events that outweigh its potential health benefits" and recommended lifestyle modifications (exercise, caloric restriction) as the primary intervention.[26] This suggests that simply replacing hormones without addressing the upstream causes of their decline (stress, EDCs, micronutrient deficiency, chronic infection) may be insufficient — consistent with the framework's own logic that root causes must be addressed.
Synthesis: The Framework's Strengths and Where It Requires Refinement
The framework's greatest strength is its internal coherence — the 5 mechanisms and 5 pathways are not independent silos but interconnected systems that amplify each other:
- Poor absorption (Mechanism 1) → impaired repair (Pathway 1) → weakened immunity (Pathway 2) → pathogen reactivation (Mechanism 3) → inflammation → further barrier damage → worse absorption
- Chronic stress (Mechanism 2) → sympathetic suppression of immunity (Pathway 2) → pathogen upregulation (Mechanism 3) → inflammation → impaired detoxification (Pathway 3) → toxin accumulation (Mechanism 4)
- Constant eating/sedentary behavior (Mechanism 5) → suppressed autophagy → impaired cellular repair (Pathway 1) → impaired detoxification (Pathway 3) → impaired metabolic health (Pathway 4)
This interconnectedness is precisely what the current ICD-coded, single-diagnosis, single-drug model fails to capture. The framework provides a physiological logic for clinical decision-making that the coding system, by design, cannot.
Where refinement may be warranted:
1. Mechanism 4 (non-infectious inflammation) could be more explicitly linked to Mechanism 3 — much of what is classified as "non-infectious" inflammation may ultimately prove to have infectious triggers that have not yet been identified, as discussed in prior conversations.
2. Pathway 4 (metabolic health) — the claim that glucose harm is "overstated" should be qualified rather than stated absolutely. The evidence supports the argument that micronutrient deficiency is an underrecognized contributor to insulin resistance, but glucose toxicity at sustained high levels is well-documented. The more precise formulation might be: the harm attributed to glucose is often the harm of the upstream conditions that produced the hyperglycemia.
3. Pathway 5 (regulatory) — the evidence on hormone replacement is genuinely mixed, and the framework should acknowledge that replacing hormones without addressing the upstream causes of their decline may produce limited benefit. The framework's own logic suggests that hormone optimization should follow, not precede, addressing the mechanisms (absorption, stress, infection, toxin burden, autophagy).
The framework represents a paradigm-level reorientation — from "what disease does this patient have?" (coding) to "which mechanisms and pathways are disrupted in this patient?" (physiology). This is precisely the shift that Genuis and Genuis (2006) called for: physicians becoming "medical sleuths, seeking to discover and deal with origins of ill-health" rather than assigning diagnostic labels and proceeding with predetermined treatment regimens.[1]
References
Exploring the continuum: medical information to effective clinical practice * . Paper II. Towards aetiology‐centred clinical practice. Genuis SJ, Genuis SK. Journal of Evaluation in Clinical Practice. 2006;12(1):63-75. doi:10.1111/j.1365-2753.2005.00609.x.
Biological and Mechanistic Pathways of Cardiometabolic Multiple Long-Term Conditions. Lim LL, Jenkins A, Prabhakaran D, et al. Lancet (London, England). 2026;:S0140-6736(26)00607-0. doi:10.1016/S0140-6736(26)00607-0.
Impaired Intestinal Barrier and Tissue Bacteria: Pathomechanisms for Metabolic Diseases. Massier L, Blüher M, Kovacs P, Chakaroun RM. Frontiers in Endocrinology. 2021;12:616506. doi:10.3389/fendo.2021.616506.
Immunology of Stress: A Review Article. Alotiby A. Journal of Clinical Medicine. 2024;13(21):6394. doi:10.3390/jcm13216394.
Glucocorticoid Resistance and Β2-Adrenergic Receptor Signaling Pathways Promote Peripheral Pro-Inflammatory Conditions Associated With Chronic Psychological Stress: A Systematic Review Across Species. Walsh CP, Bovbjerg DH, Marsland AL. Neuroscience and Biobehavioral Reviews. 2021;128:117-135. doi:10.1016/j.neubiorev.2021.06.013.
Autonomic Nervous System and Neuroimmune Interactions: New Insights and Clinical Implications. Benarroch EE. Neurology. 2019;92(8):377-385. doi:10.1212/WNL.0000000000006942.
An Overview of the Role of Sympathetic Regulation of Immune Responses in Infectious Disease and Autoimmunity. Bucsek MJ, Giridharan T, MacDonald CR, Hylander BL, Repasky EA. International Journal of Hyperthermia : The Official Journal of European Society for Hyperthermic Oncology, North American Hyperthermia Group. 2018;34(2):135-143. doi:10.1080/02656736.2017.1411621.
Health Effects of Fossil Fuel–Derived Endocrine Disruptors. Woodruff TJ. The New England Journal of Medicine. 2024;390(10):922-933. doi:10.1056/NEJMra2300476.
Endocrine-Disrupting Chemicals: Mainstream Recognition of Health Effects and Implications for the Practicing Internist. Trasande L, Sargis RM. Journal of Internal Medicine. 2024;295(2):259-274. doi:10.1111/joim.13748.
Effects of Intermittent Fasting on Health, Aging, and Disease. de Cabo R, Mattson MP. The New England Journal of Medicine. 2019;381(26):2541-2551. doi:10.1056/NEJMra1905136.
Interplay Between Autophagy, Cellular Senescence, and Brain Aging: Neuroprotective Implications of Intermittent Fasting. Singh I, Bhat S, Tamatta R, Singh AK. Cellular and Molecular Neurobiology. 2026;46(1):75. doi:10.1007/s10571-026-01709-7.
Vitamin D in Autophagy Signaling for Health and Diseases: Insights on Potential Mechanisms and Future Perspectives. Bhutia SK. The Journal of Nutritional Biochemistry. 2022;99:108841. doi:10.1016/j.jnutbio.2021.108841.
Autophagy as a Basis for the Health-Promoting Effects of Vitamin D. Høyer-Hansen M, Nordbrandt SP, Jäättelä M. Trends in Molecular Medicine. 2010;16(7):295-302. doi:10.1016/j.molmed.2010.04.005.
Protective role of vitamin D against oxidative stress in diabetic retinopathy. Valle MS, Russo C, Malaguarnera L. Diabetes/Metabolism Research and Reviews. 2021;37(8):e3447. doi:10.1002/dmrr.3447.
From Development to Aging: Dynamic Roles of the Thymic Medulla in T Cell Biology. Michalaki C, Sharjeel M, Cowan JE. Immunological Reviews. 2026;339(1):e70118. doi:10.1111/imr.70118.
Role of Thymus in Health and Disease. Gulla S, Reddy MC, Reddy VC, et al. International Reviews of Immunology. 2023;42(5):347-363. doi:10.1080/08830185.2022.2064461.
Age-Related Thymic Involution: Mechanisms and Functional Impact. Liang Z, Dong X, Zhang Z, Zhang Q, Zhao Y. Aging Cell. 2022;21(8):e13671. doi:10.1111/acel.13671.
Targeting Gut-Liver-Kidney Axis: Microbiota-Derived Metabolites and Therapeutic Implications. Zhang Y, Sun C, Wang Y, et al. Cell Communication and Signaling : CCS. 2026;:10.1186/s12964-025-02625-x. doi:10.1186/s12964-025-02625-x.
Lymphatic Dysfunction in Advanced Cirrhosis: Contextual Perspective and Clinical Implications. Kumar R, Anand U, Priyadarshi RN. World Journal of Hepatology. 2021;13(3):300-314. doi:10.4254/wjh.v13.i3.300.
The Consumption of Micronutrients in Relation to Calorie Intake and Risk of Insulin Resistance. Piyathilake CJ, Badiga S, Hernandez A, Brill IK, Jolly PE. Nutrition, Metabolism, and Cardiovascular Diseases : NMCD. 2022;32(6):1385-1391. doi:10.1016/j.numecd.2022.02.007.
Excessive Refined Carbohydrates and Scarce Micronutrients Intakes Increase Inflammatory Mediators and Insulin Resistance in Prepubertal and Pubertal Obese Children Independently of Obesity. López-Alarcón M, Perichart-Perera O, Flores-Huerta S, et al. Mediators of Inflammation. 2014;2014:849031. doi:10.1155/2014/849031.
The Role of Mineral Deficiencies in Insulin Resistance and Obesity. Smita RM, Shuvo APR, Raihan S, et al. Current Diabetes Reviews. 2022;18(7):e171121197987. doi:10.2174/1573399818666211117104626.
Insulin Resistance: An Adaptive Mechanism Becomes Maladaptive in the Current Environment - An Evolutionary Perspective. Tsatsoulis A, Mantzaris MD, Bellou S, Andrikoula M. Metabolism: Clinical and Experimental. 2013;62(5):622-33. doi:10.1016/j.metabol.2012.11.004.
Vitamin D Deficiency Induces Insulin Resistance and Re-Supplementation Attenuates Hepatic Glucose Output via the PI3K-AKT-FOXO1 Mediated Pathway. Mutt SJ, Raza GS, Mäkinen MJ, et al. Molecular Nutrition & Food Research. 2020;64(1):e1900728. doi:10.1002/mnfr.201900728.
Hormones and Aging: An Endocrine Society Scientific Statement. Cappola AR, Auchus RJ, El-Hajj Fuleihan G, et al. The Journal of Clinical Endocrinology and Metabolism. 2023;108(8):1835-1874. doi:10.1210/clinem/dgad225.
Hormonal and Metabolic Changes of Aging and the Influence of Lifestyle Modifications. Pataky MW, Young WF, Nair KS. Mayo Clinic Proceedings. 2021;96(3):788-814. doi:10.1016/j.mayocp.2020.07.033.
The Physiology of Endocrine Systems With Ageing. van den Beld AW, Kaufman JM, Zillikens MC, et al. The Lancet. Diabetes & Endocrinology. 2018;6(8):647-658. doi:10.1016/S2213-8587(18)30026-3.
Anti-Aging Effects of the Adrenal Androgens Dehydroepiandrosterone and Dehydroepiandrosterone Sulfate: Mechanisms of Action and Beneficial Effects in Older People. Nawata H, Yanase T, Morohashi KI, Nomura M, Muta K. Endocrine Journal. 2026;73(4):495-516. doi:10.1507/endocrj.EJ25-0483.
DHEA in Elderly Women and DHEA or Testosterone in Elderly Men. Nair KS, Rizza RA, O'Brien P, et al. The New England Journal of Medicine. 2006;355(16):1647-59. doi:10.1056/NEJMoa054629.
Let's come up with a better way. How about basing clinical decisions on physiology rather than symptomatic coding? I would like you to comment on what I have developed. I believe most diseases, especially chronic diseases, can be understood at the root-cause level and thus effectively treated or otherwise intervened upon by evaluating 5 mechanisms of disease and 5 pathways. (To see the full question, go to the bottom of this blog.)
Here is their answer in its entirety. It is NOT light reading. Once you grasp these concepts, you will understand your own health far better than any doctor.
Here is what I asked the Harvard/MIT AI - OpenEvidence - to find out what it thought of the coding system (previous blog) and what it thought about the concept of mechanisms and pathways as a way forward to improve healthcare delivery. Yes, HEALTHcare, NOT SICKcare!
Updates
Get low- and no-cost health tips and root-cause solutions.
FrugalDoc
Affordable Health & Wellness
© 2025 FrugalDoc Health & Wellness. All rights reserved.