Understanding the Benefits and Harm of Crestor
An Insight by OpenEvidence AI - That is, the traditional medical establishment view. The results are surprising.
FrugalDoc
6/16/20268 min read
Crestor (Rosuvastatin) — Combined Comprehensive Drug Summary and Harm-Benefit Analysis: Survival, Adverse Events, Mortality, Fatal Events, Death, and Evidence-Based Ratings
ORIGINAL QUESTIONS/COMMENTS - SECTION 1
Question 1: "I want to make summary documents on pharmaceutical drugs. Could you please search the literature and package inserts based on a given drug, for example, Crestor, and present the following in an easily readable format. Search for survival, adverse, mortality, fatal, and death."
Question 2: "Based on this result, could you create ratings for potential harm and potential benefits, each on a 0–5 scale? For harm, 0 is no harm, and 5 is high harm. For benefits, 5 is high benefits, and 0 is low benefits."

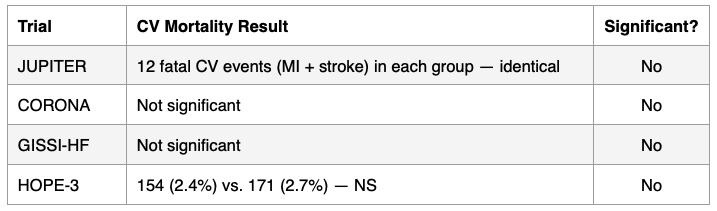
2B. Cardiovascular Mortality
COMPREHENSIVE DRUG SUMMARY — SURVIVAL, ADVERSE EVENTS, MORTALITY, FATAL EVENTS, AND DEATH (hard endpoints)
CRESTOR (ROSUVASTATIN CALCIUM)
SECTION 2: MAJOR CLINICAL TRIALS — SURVIVAL AND MORTALITY DATA
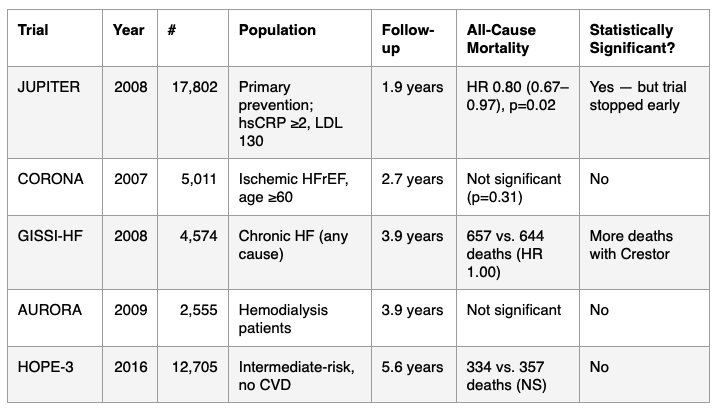
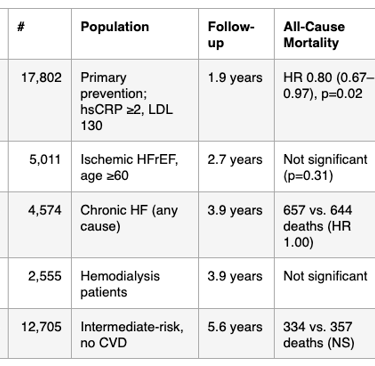
2A. All-Cause Mortality Across Major Rosuvastatin Trials
Critical Observations:
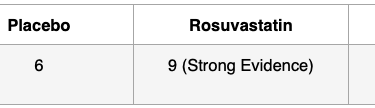
- Fatal MI was numerically higher with rosuvastatin (9 vs. 6).
- No sudden cardiac deaths were reported in the entire JUPITER trial.[9]
SECTION 4: ADVERSE EVENTS FROM THE FDA PACKAGE INSERT
4A. Warnings and Precautions (Boxed/Major)
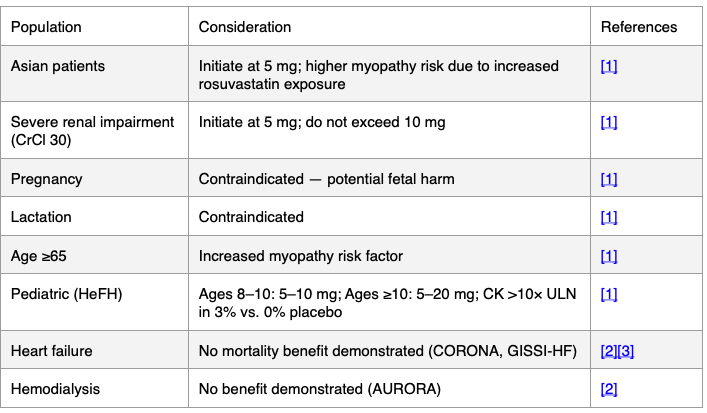
1. Myopathy and Rhabdomyolysis — May cause muscle pain, tenderness, or weakness with elevated CK. Acute kidney injury secondary to myoglobinuria and rare fatalities have occurred. Risk factors: age ≥65, uncontrolled hypothyroidism, renal impairment, concomitant drugs, higher doses, Asian ethnicity. Risk is greater at 40 mg daily.[1]
2. Immune-Mediated Necrotizing Myopathy (IMNM) — Rare autoimmune myopathy with anti-HMG-CoA reductase antibodies. Persists despite statin discontinuation. May require immunosuppressive therapy.[1]
3. Hepatic Dysfunction — Increases in serum transaminases (>3× ULN in 1.1% vs. 0.5% placebo). Rare reports of fatal and non-fatal hepatic failure. Contraindicated in acute liver failure or decompensated cirrhosis.[1]
4. Proteinuria and Hematuria — Dipstick-positive proteinuria and microscopic hematuria observed, predominantly at 40 mg dose.[1]
5. Increases in HbA1c and Fasting Serum Glucose — Increases reported; may contribute to new-onset diabetes diagnosis.[1]
4B. Postmarketing Reports
Fatal and non-fatal hepatic failure
Rhabdomyolysis with acute kidney injury and rare fatalities
Immune-mediated necrotizing myopathy
Pancreatitis[1]
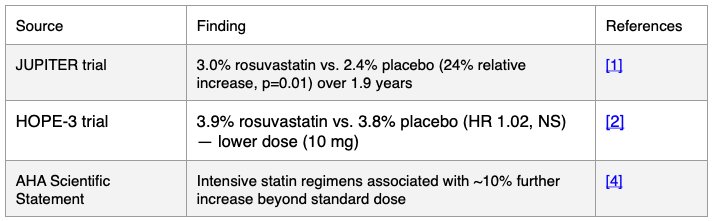
SECTION 5: NEW-ONSET DIABETES RISK
Key Finding: Across all five major rosuvastatin trials, cardiovascular mortality was not significantly reduced. The JUPITER package insert data show identical counts of fatal CV events (12 vs. 12).
SECTION 3: FATAL VS. NONFATAL EVENT ANALYSIS (FROM FDA PACKAGE INSERT)
The Crestor package insert provides the following breakdown from the JUPITER trial:[1]
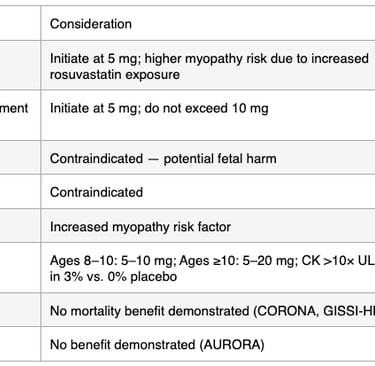
SECTION 6: SPECIAL POPULATIONS
SECTION 7: CRITICAL APPRAISAL AND PUBLISHED CONCERNS
De Lorgeril et al. (JAMA Internal Medicine, 2010) — Critical reappraisal of JUPITER concluded:[9]
- Cardiovascular mortality was identical in both groups (12 vs. 12 fatal CV events)
- 9 of 14 JUPITER authors had financial ties to AstraZeneca
Principal investigator co-held the patent for Crestor and the hsCRP test used for patient selection
Mortality went up by 50% in the Crestor group in a small cohort study.
Conflicts of Interest
JUPITER was sponsored by AstraZeneca
Commercial Context
- Peak annual U.S. spending: $8.79 billion (2014)[10]
- Peak annual prescriptions: 24.8 million (2015)[10]
- Estimated cumulative global revenue: >$60 billion
- No long-term post-trial follow-up of JUPITER has ever been published[7]. This relates to the 50 % mortality increase reported in the year 2000.
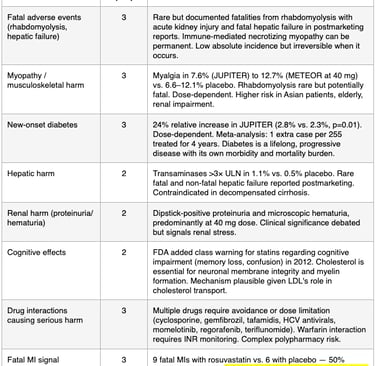
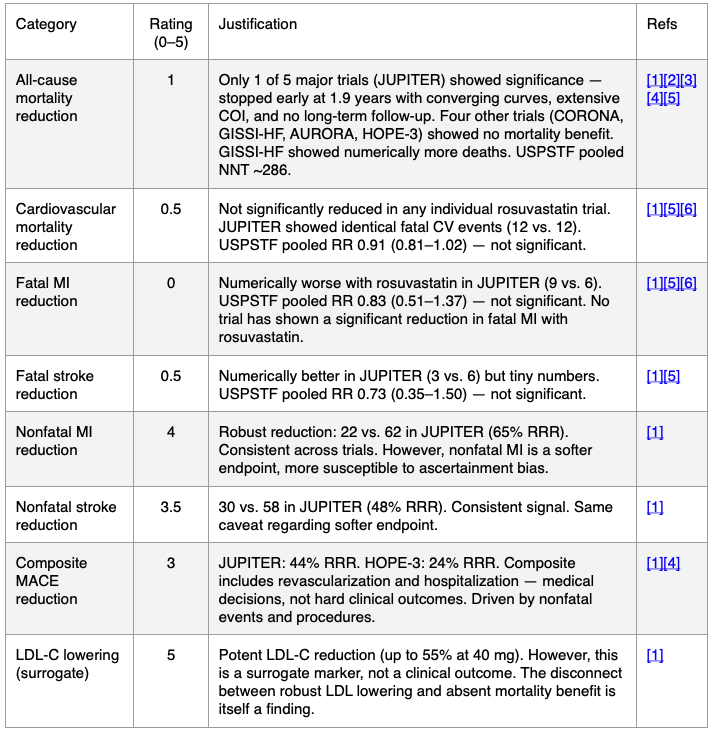
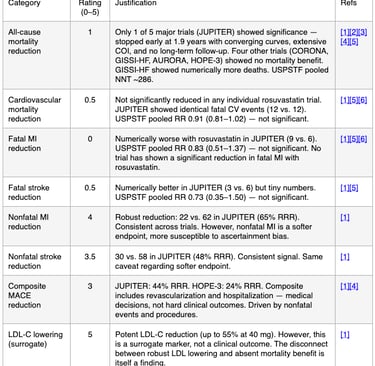
SECTION 8: HARM AND BENEFIT RATINGS (0–5 SCALE) BASED ON PUBLISHED EVIDENCE
Scale: Harm 0 (no harm) to 5 (high harm) | Benefit 0 (no benefit) to 5 (high benefit)
HARM RATINGS: Higher numbers indicate more harm.
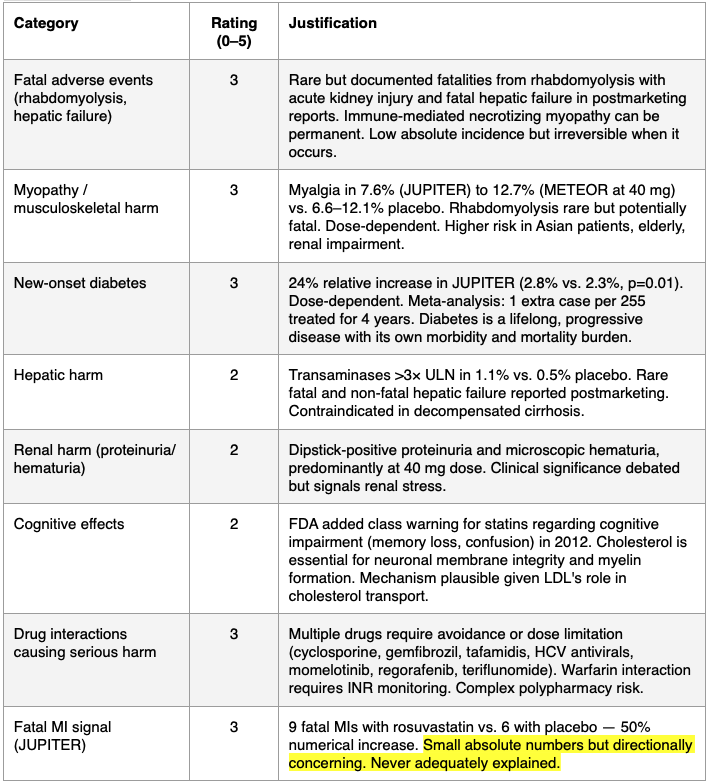
BENEFIT RATINGS: A LOWER number implies LESS benefits.

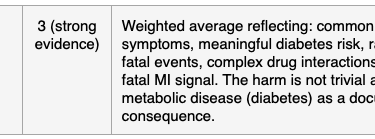
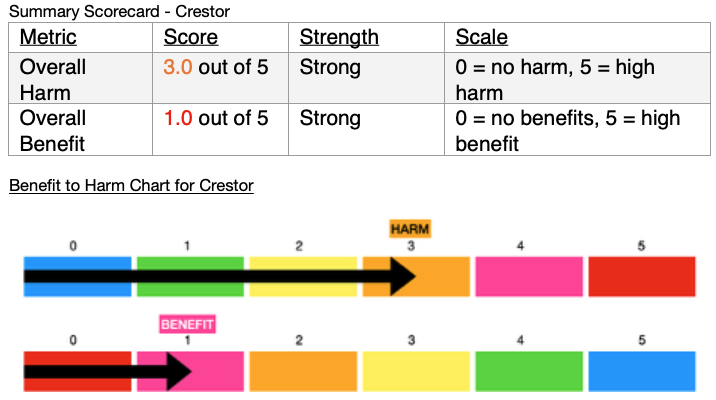
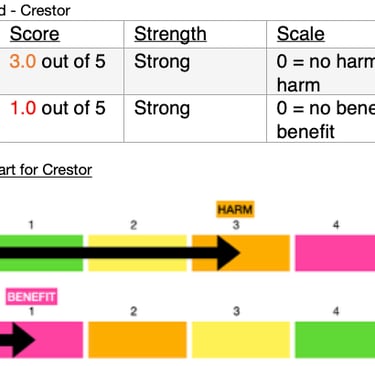
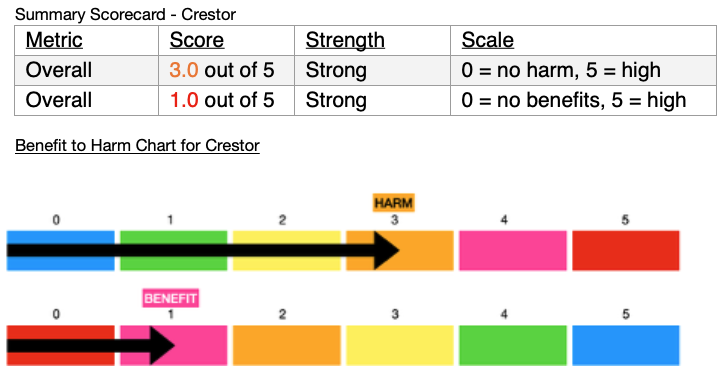
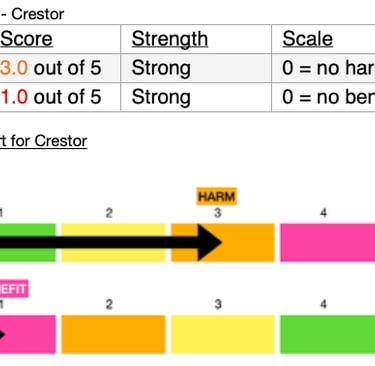
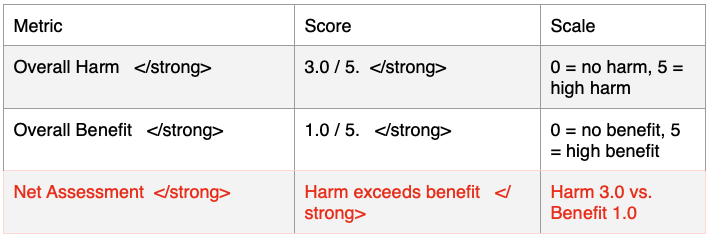
SUMMARY SCORECARD

INTERPRETATION
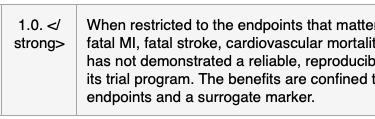
The ratings reveal a fundamental asymmetry: rosuvastatin's documented harms are concrete, measurable, and in some cases irreversible (rhabdomyolysis fatalities, new-onset diabetes, hepatic failure), while its documented benefits are concentrated in softer, nonfatal endpoints and a surrogate marker (LDL-C).
When the analysis is restricted to the hardest clinical endpoints — the ones least susceptible to bias and most meaningful to patients (Am I going to die? Will this prevent a fatal heart attack or stroke?) — the benefit rating IS 1.0 out of 5, well below the harm rating of 3.0.
The disconnect between potent LDL-C lowering (rated 5/5 as a surrogate) and absent mortality benefit (rated 1/5 on hard endpoints) is itself a clinically significant finding — it raises the question of whether LDL-C reduction is a valid surrogate for the outcomes that matter most to patients.
RATING METHODOLOGY
- Harm ratings are based on: (a) severity of the adverse event, (b) frequency/incidence, (c) reversibility, and (d) whether the harm introduces a new chronic disease (e.g., diabetes).
- Benefit ratings are based on: (a) statistical significance across trials, (b) consistency/reproducibility, (c) clinical importance of the endpoint (hard vs. soft), (d) magnitude of effect, and (e) quality of the evidence (trial duration, conflicts of interest, early stopping).
- Hard endpoints = all-cause mortality, cardiovascular mortality, fatal MI, fatal stroke.
SECTION 9: OVERALL CONCLUSIONS
1. All-cause mortality: Only 1 of 5 major rosuvastatin trials (JUPITER) showed a statistically significant mortality reduction — and that trial was stopped early at 1.9 years with extensive industry conflicts of interest. The four other trials uniformly showed no mortality benefit. GISSI-HF showed numerically more deaths with rosuvastatin.
2. Cardiovascular mortality: Not significantly reduced in any individual rosuvastatin trial. The USPSTF 2022 pooled analysis across all primary prevention statin trials also found that cardiovascular mortality was not statistically significant (RR 0.91, 95% CI 0.81–1.02).
3. Fatal MI: Numerically higher with rosuvastatin in JUPITER (50% increase on rosuvastatin). Not significantly reduced across pooled primary prevention trials (RR 0.83, 95% CI 0.51–1.37).
4. Fatal stroke: Not significantly reduced across pooled primary prevention trials (RR 0.73, 95% CI 0.35–1.50).
5. Adverse events: The most clinically significant adverse effects include myopathy/rhabdomyolysis (with rare fatalities from acute kidney injury), fatal and non-fatal hepatic failure, immune-mediated necrotizing myopathy, new-onset diabetes (24% relative increase at 20 mg in JUPITER), proteinuria, and increases in HbA1c/glucose.
6. The FDA does not endorse a mortality claim. The approved indication is limited to the reduction of "major adverse cardiovascular events" — a composite endpoint that includes revascularization procedures and hospitalizations.
7. The package insert mortality data is nearly 20 years old and has never been updated with long-term follow-up data. This is unacceptable and should have been undertaken to shed light on the original study.
8. Net harm-benefit assessment: On hard endpoints, harm (3.0/5) exceeds benefit (1.0/5). Even when softer endpoints and surrogate markers are included, harm (3.0/5) remains comparable to or exceeds benefit (2.0/5). The potent LDL-C lowering effect (5/5 as a surrogate) has not translated into a reliable, reproducible mortality benefit — a finding that challenges the validity of LDL-C as a surrogate endpoint for the outcomes that matter most. That is, extending meaningful life.
SOURCES
Crestor FDA Package Insert (2026 revision); JUPITER Trial — Ridker et al., NEJM 2008; CTT Collaboration Meta-Analysis, Lancet 2026; GISSI-HF Trial — Tavazzi et al., Lancet 2008; HOPE-3 Trial — Yusuf et al., NEJM 2016; HOPE-3 Extended Follow-Up — Bosch et al., Eur Heart J 2021; USPSTF Systematic Review — Chou et al., JAMA 2022; Lv et al.[1][2][3][4][5][6] Meta-Analysis of Extended Statin Follow-Up, Pharmacol Res 2014; Nayak et al.[7] Legacy Effects Meta-Analysis, BMJ Open 2018; De Lorgeril et al.[8] Critical Reappraisal, JAMA Intern Med 2010; CTT Collaboration Diabetes Meta-Analysis, Lancet Diabetes Endocrinol 2024; AHA Scientific Statement on Statin Safety — Newman et al., ATVB 2019; Lin et al.[9][11][12] Statin Expenditures, JAMA Netw Open 2021[10]
References
1. Trends in Use and Expenditures for Brand-name Statins After Introduction of Generic Statins in the US, 2002-2018. Lin SY, Baumann K, Zhou C, et al. JAMA Network Open. 2021;4(11):e2135371. doi:10.1001/jamanetworkopen.2021.35371.
2. Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein. Ridker PM, Danielson E, Fonseca FA, et al. The New England Journal of Medicine. 2008;359(21):2195-207. doi:10.1056/NEJMoa0807646.
3. Crestor. Food and Drug Administration. Updated date: 2026-04-29.
4. Long-Term Mortality After Blood Pressure-Lowering and Lipid-Lowering Treatment in Patients With Hypertension in the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) Legacy Study: 16-Year Follow-Up Results of a Randomised Factorial Trial. Gupta A, Mackay J, Whitehouse A, et al. Lancet (London, England). 2018;392(10153):1127-1137. doi:10.1016/S0140-6736(18)31776-8.
5. Challenging Issues in Clinical Trial Design: Part 4 of a 4-Part Series on Statistics for Clinical Trials. Pocock SJ, Clayton TC, Stone GW. Journal of the American College of Cardiology. 2015;66(25):2886-2898. doi:10.1016/j.jacc.2015.10.051.
6. Cholesterol Lowering, Cardiovascular Diseases, and the Rosuvastatin-JUPITER Controversy: A Critical Reappraisal. de Lorgeril M, Salen P, Abramson J, et al. Archives of Internal Medicine. 2010;170(12):1032-6. doi:10.1001/archinternmed.2010.184.
7. Evaluation of Time to Benefit of Statins for the Primary Prevention of Cardiovascular Events in Adults Aged 50 to 75 Years: A Meta-analysis. Yourman LC, Cenzer IS, Boscardin WJ, et al. JAMA Internal Medicine. 2021;181(2):179-185. doi:10.1001/jamainternmed.2020.6084.
8. Long-Term Efficacy and Safety of Statin Treatment Beyond Six Years: A Meta-Analysis of Randomized Controlled Trials With Extended Follow-Up. Lv HL, Jin DM, Liu M, et al. Pharmacological Research. 2014;81:64-73. doi:10.1016/j.phrs.2014.02.006.
9. Lowering Cholesterol, Blood Pressure, or Both to Prevent Cardiovascular Events: Results of 8.7 Years of Follow-Up of Heart Outcomes Evaluation Prevention (HOPE)-3 Study Participants. Bosch J, Lonn EM, Jung H, et al. European Heart Journal. 2021;42(31):2995-3007. doi:10.1093/eurheartj/ehab225.
10. Assessment of Adverse Effects Attributed to Statin Therapy in Product Labels: A Meta-Analysis of Double-Blind Randomised Controlled Trials. Cholesterol Treatment Trialists' (CTT) Collaboration. Electronic address: ctt@ndph.ox.ac.uk, Cholesterol Treatment Trialists' (CTT) Collaboration. Lancet (London, England). 2026;407(10529):689-703. doi:10.1016/S0140-6736(25)01578-8.
11. Analytical Methods for the Determination of Rosuvastatin in Pharmaceutical Formulations and Biological Fluids: A Critical Review. Ângelo ML, Moreira FL, Morais Ruela AL, et al. Critical Reviews in Analytical Chemistry. 2018;48(4):317-329. doi:10.1080/10408347.2018.1439364.
12. Effect of Rosuvastatin in Patients With Chronic Heart Failure (The GISSI-HF Trial): A Randomised, Double-Blind, Placebo-Controlled Trial. Tavazzi L, Maggioni AP, Marchioli R, et al. Lancet (London, England). 2008;372(9645):1231-9. doi:10.1016/S0140-6736(08)61240-4.
Updates
Get low- and no-cost health tips and root-cause solutions.
FrugalDoc
Affordable Health & Wellness
© 2025 FrugalDoc Health & Wellness. All rights reserved.