Understanding OPTIMAL LDL Levels Across Your Lifespan
LDL is part of your fundamental repair process. Thus, younger people tend to have lower LDL levels, while older people, whose immune system is in decline, need more repair, thus higher levels of LDL.
FrugalDoc
6/18/202612 min read
LDL, the most demonized of all naturally produced substances, is simply a SOAP!
LDL Levels Across Age Groups and the Role of LDL as a Repair Transport Vehicle in Aging — A Discussion
Original Question 1: "Please provide information on LDL levels across various age groups, like 20-29. Please only use population-based studies. Also, explain why the oldest populations break the trend due to statin use."
Original Question 2: "Explain why LDL is higher in older populations..”
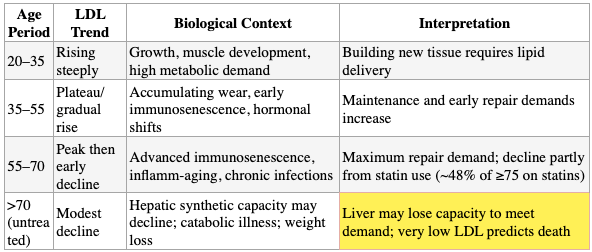
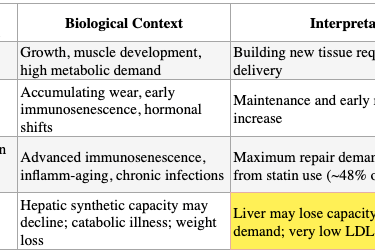
The Core Point: The body does not produce more of a vital transport molecule by accident. LDL rises with age because aging tissues — battered by immunosenescence, chronic inflammation, oxidative stress, and microbial burden — require more phospholipids, cholesterol, fatty acids, and fat-soluble vitamins for membrane repair, cell replacement, hormone synthesis, and immune defense.
Part 1: Population-Based LDL Levels by Age Group
LDL levels rise progressively from young adulthood through middle age, then decline in the oldest age groups — a pattern consistently observed across multiple large population-based studies. The decline in the elderly is driven by a combination of widespread statin use, survivorship bias, reverse causation from catabolic illness, and genuine physiological changes in lipid metabolism.
NHANES (U.S., 1999–2002) — This nationally representative survey of U.S. adults provides age- and sex-specific mean LDL values:[1]
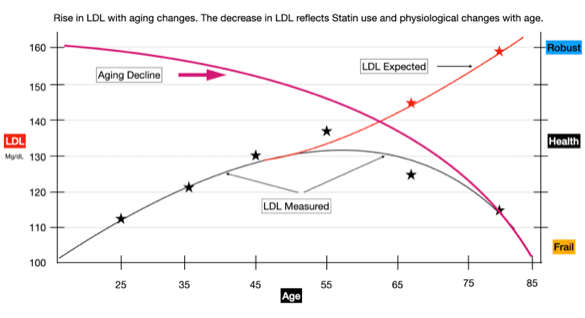
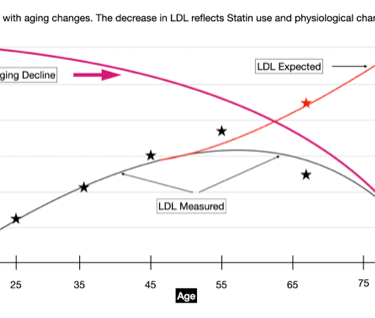
Here is a graphical representation of the chart above.
Note the correlation between rising LDL levels and increased age. The inflection point has two (2) major contributors.
Statin and LDL-lowering drug use.
Age-related changes in physiology, including LDL production.
The purple curve is an estimate of the declining health in aging populations. Note how aging accelerates alongside a similar decline in LDL, consistent with population mortality data
Could supplementing with lipoproteins, including LDL, be an intervention to slow aging? The curves above indicate it is possible.
Dutch Lifelines Study (133,450 participants, no lipid-lowering drug use) — This study excluded all individuals on lipid-lowering medications, making it uniquely valuable for understanding the natural trajectory. In men, LDL increased 64% (median +54 mg/dL) from age 20 to 49. In women, LDL was stable from 18 to 35, then increased 42% (median +42 mg/dL) through age 59.[2
Chinese Population Study (84,285 participants) — In men, LDL increased with age through ~60 years, then declined. In women, LDL increased through ~60 years, then declined. The turning point was approximately age 60 for both sexes.[3]
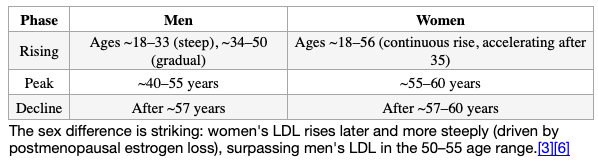
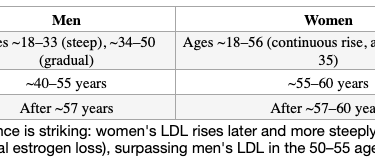
Zhang et al. (84,285 participants, China) — This study plotted LDL at one-year age increments from 18 to 85 and found the trajectory is nonlinear: in males, LDL rose steeply from 18–33, plateaued from 34–56, then declined after 57. In females, LDL rose continuously from 18–56, then declined after 57.[4]
Global Diagnostics Network (461 million lipid results, 17 countries) — Across five continents, LDL peaked at 40–49 years in males and 50–59 years in females in most countries.[5]
The Natural Pattern: Rise, Peak, Decline
Why the Oldest Age Groups Break the Trend
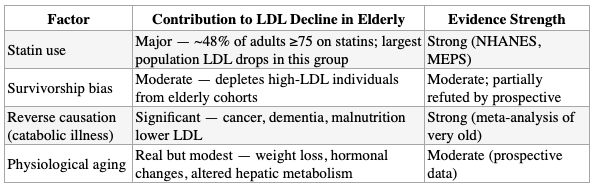
The decline in LDL after age ~60 is real and reproducible, but its interpretation is complicated by multiple confounders.
1. Statin Use Is Extremely Prevalent in Older Adults
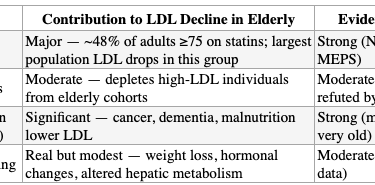
NHANES data show that nearly half (47.6%) of adults ≥75 years in the U.S. use prescription cholesterol-lowering medications, with >80% using a statin alone.[7] Among adults ≥80 years, primary prevention statin use increased from ~9% in 1999–2000 to 34% in 2011–2012.[7] This massive pharmacologic intervention artificially suppresses population-level LDL values in the oldest groups. The NHANES trend data from 1988–2002 showed the largest LDL decreases occurred in the ≥75 age group for both men and women — precisely the period when statin prescribing exploded.[1]
2. Survivorship Bias
Individuals with lifelong underlying health problems leading to expression of high LDL who were susceptible to ASCVD may have died before reaching old age, depleting the high-LDL individuals from the surviving elderly population and lowering the group mean.[6][8][9] However, the Rancho Bernardo Study (1,041 men, 1,303 women, ages 50–93) followed participants prospectively for 8 years and found that LDL decreased approximately 1% per year in both sexes — even after excluding those on lipid-lowering drugs. The authors concluded that the cross-sectional decline in men is not fully explained by survivorship bias because it is also observed prospectively within individuals.[10]
3. Reverse Causation and Catabolic Illness
Low LDL in the very old may reflect underlying catabolic conditions — cancer, renal disease, dementia, malnutrition, and weight loss — all of which lower LDL and increase mortality risk.[6][9] A meta-analysis of individual patient data from 2,317 very old adults (median age 85) found an inverse association between LDL and 5-year mortality (HR 0.87 per 1 mmol/L increase), most pronounced in those with low composite fitness scores (HR 0.85), suggesting that the "protective" effect of higher LDL in the very old is largely driven by reverse causation — sicker people have lower LDL.[11]
4. Genuine Physiological Changes
Even after accounting for statins, survivorship, and illness, there appear to be real age-related changes in lipid metabolism: decreased hepatic LDL receptor activity, altered body composition, insulin resistance, and decreased growth hormone all contribute to changes in lipid profiles with aging.[6] Weight change was the single most important predictor of LDL change in the Rancho Bernardo prospective analysis.[10]
Summary: Disentangling the Elderly LDL Decline
Part 2: LDL as a Transport Vehicle — Why Elevation in Older Populations Reflects Repair Demand
LDL: A Delivery Vehicle, Not a Toxin
LDL's core biological function is to transport processed cholesterol, fatty acids, triglycerides, phospholipids, and fat-soluble vitamins from the liver to peripheral tissues for membrane synthesis, steroid hormone production, and energy supply.[12] LDL particles carry hydrophobic cholesteryl esters and triglycerides in a central core, enveloped by an external layer of hydrophilic phospholipids and free cholesterol, functioning as a soap-like emulsification system that solubilizes fats in the aqueous bloodstream.
At the cellular level, the evidence is remarkably specific:
- LDL delivers cholesterol to the plasma membrane via receptor-mediated endocytosis → lysosomal hydrolysis → Rab8a/Myosin5b-dependent transport to the cell surface, where it is incorporated into the phospholipid bilayer. This cholesterol is essential for membrane integrity, fluidity, and function.[13][14]
- LDL delivers vitamin E (tocopherol) to cells via the LDL receptor — cells with defective LDL receptors (familial hypercholesterolemia) receive only ~38% of the vitamin E that normal cells receive.[15]
- LDL directly stimulates wound healing through SR-BI receptor-mediated activation of p38 MAPKs, increasing cell migration and wound closure capacity.[16]
- LDL deposits phospholipids into cell membranes even in the absence of LDL receptors, through calcium-dependent adsorption — a mechanism for direct membrane repair.[17]
Immunosenescence and the Demand-Side Argument
With aging, the immune system undergoes profound deterioration — termed "inflamm-aging" — characterized by irreversible cell cycle arrest (cellular senescence), accumulation of senescence-associated secretory phenotype (SASP) cells that produce inflammatory mediators, dysregulation of both innate and adaptive immunity, and increased vulnerability to infections and chronic disease.[18] This process damages endothelial cells, vascular smooth muscle, organ parenchyma, and connective tissue throughout the body. Every damaged cell membrane requires phospholipids and cholesterol for repair. Every new cell replacing a dead one requires a complete phospholipid bilayer. The delivery vehicle for these materials is LDL.
The logic follows: more damage → more repair needed → more building materials required → more LDL produced and circulated. This is not a pathological overproduction — it is a proportional response to increased demand.
The Mortality Data Support This Interpretation
If LDL were inherently harmful, higher LDL should predict higher mortality at every age. It does not. The data consistently show the opposite in older populations:
- Copenhagen General Population Study (108,243 individuals): The LDL concentration associated with the lowest all-cause mortality was 3.6 mmol/L (140 mg/dL) — well above guideline targets. LDL below 1.8 mmol/L (<70 mg/dL) carried a 25% increased mortality risk compared to the 132–154 mg/dL range.[19]
- ASPREE Trial (12,334 healthy adults ≥65 years, not on statins): U-shaped relationship between LDL and all-cause mortality, with the nadir at 3.3–3.4 mmol/L (127–131 mg/dL). Each 1 mmol/L higher LDL was associated with 9% lower all-cause mortality, 16% lower cancer mortality, and 18% lower non-CVD/non-cancer mortality.[20]
- Systematic review of 19 cohort studies (68,094 elderly): Inverse association between LDL and all-cause mortality in 16 of 28 cohorts (92% of participants) — higher LDL was associated with living longer.[21]
- Individual patient data meta-analysis (2,317 very old adults, median age 85): Each 1 mmol/L increase in LDL was associated with 13% lower 5-year mortality (HR 0.87), most pronounced in those with the lowest fitness scores — precisely the individuals with the most tissue damage and repair needs.[11]
- Shanghai Aging Study (3,239 older adults, 10-year follow-up): The lowest LDL quintile (<2.61 mmol/L) had 67% higher mortality than the highest quintile (≥4.10 mmol/L), even after excluding early deaths and functionally impaired participants.[22]
LDL's Immune Defense Role
Beyond membrane repair, LDL participates directly in innate immune defense. LDL binds and neutralizes bacterial lipopolysaccharide (LPS) — the endotoxin from gram-negative bacteria that triggers severe inflammatory responses.[23][24]
LPS-binding protein (LBP) circulates in association with LDL and VLDL in healthy individuals, and this LBP-LDL complex strongly enhances LPS scavenging capacity.[24] During sepsis, when HDL levels drop, LDL and VLDL become the predominant LPS-binding lipoproteins, serving as a critical backup defense system.[23][24]
Fat accumulation, including LDL and the actual cholesterol molecule in macrophages and immune cells, augments Toll-like receptor signaling, inflammasome activation, and production of monocytes and neutrophils — responses that, while potentially harmful in chronic excess, are fundamentally beneficial for fighting infections.[25]
The Integrated Framework
The Core Point
The body does not produce more of a vital transport molecule by accident. LDL rises with age because aging tissues — battered by immunosenescence, chronic inflammation, oxidative stress, and microbial burden — require more phospholipids, cholesterol, fatty acids, and fat-soluble vitamins for membrane repair, cell replacement, hormone synthesis, and immune defense.
The mortality data among the elderly consistently show that those with higher LDL levels live longer, particularly those in the worst health — exactly the pattern expected if LDL serves a reparative and protective function rather than causing harm
Pharmacologically suppressing this transport system in older adults, without addressing the underlying damage driving the demand, removes the building materials without fixing the building.
References
Question 1
Trends in Serum Lipids and Lipoproteins of Adults, 1960-2002. Carroll MD, Lacher DA, Sorlie PD, et al. JAMA. 2005;294(14):1773-81. doi:10.1001/jama.294.14.1773.
Lipid and Lipoprotein Reference Values From 133,450 Dutch Lifelines Participants: Age- And Gender-Specific Baseline Lipid Values and Percentiles. Balder JW, de Vries JK, Nolte IM, et al. Journal of Clinical Lipidology. 2017 Jul - Aug;11(4):1055-1064.e6. doi:10.1016/j.jacl.2017.05.007.
Age-Related Trends in Lipid Levels: A Large-Scale Cross-Sectional Study of the General Chinese Population. Feng L, Nian S, Tong Z, et al. BMJ Open. 2020;10(3):e034226. doi:10.1136/bmjopen-2019-034226.
Trends in LDL-C and Non-HDL-C Levels With Age. Zhang P, Su Q, Ye X, et al. Aging and Disease. 2020;11(5):1046-1057. doi:10.14336/AD.2019.1025.
Lipid Distributions in the Global Diagnostics Network Across Five Continents. Martin SS, Niles JK, Kaufman HW, et al. European Heart Journal. 2023;44(25):2305-2318. doi:10.1093/eurheartj/ehad371.
Life's Essential 8: Optimizing Health in Older Adults. Kumar M, Orkaby A, Tighe C, et al. JACC. Advances. 2023;2(7):100560. doi:10.1016/j.jacadv.2023.100560.
Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: US Preventive Services Task Force Recommendation Statement. US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, et al. JAMA. 2016;316(19):1997-2007. doi:10.1001/jama.2016.15450.
Altered Cardiovascular Risk Pattern of LDL Cholesterol in Older Adults. Rozing MP, Westendorp RGJ. Current Opinion in Lipidology. 2023;34(1):22-26. doi:10.1097/MOL.0000000000000859.
National Lipid Association Annual Summary of Clinical Lipidology 2015. Bays HE, Jones PH, Brown WV, Jacobson TA. Journal of Clinical Lipidology. 2014 Nov-Dec;8(6 Suppl):S1-36. doi:10.1016/j.jacl.2014.10.002.
Total, LDL, and HDL Cholesterol Decrease With Age in Older Men and Women. The Rancho Bernardo Study 1984-1994. Ferrara A, Barrett-Connor E, Shan J. Circulation. 1997;96(1):37-43. doi:10.1161/01.cir.96.1.37.
The Role of a Composite Fitness Score in the Association Between Low-Density Cholesterol and All-Cause Mortality in Older Adults: An Individual Patient Data Meta-Analysis. van der Ploeg MA, Poortvliet RKE, Bogaerts JMK, et al. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2023;78(9):1708-1716. doi:10.1093/gerona/glad148.
LDL Cholesterol: Controversies and Future Therapeutic Directions. Ridker PM. Lancet (London, England). 2014;384(9943):607-617. doi:10.1016/S0140-6736(14)61009-6.
Last Step in the Path of LDL Cholesterol From Lysosome to Plasma Membrane to ER Is Governed by Phosphatidylserine. Trinh MN, Brown MS, Goldstein JL, et al. Proceedings of the National Academy of Sciences of the United States of America. 2020;117(31):18521-18529. doi:10.1073/pnas.2010682117.
LDL Cholesterol Recycles to the Plasma Membrane via a Rab8a-Myosin5b-Actin-Dependent Membrane Transport Route. Kanerva K, Uronen RL, Blom T, et al. Developmental Cell. 2013;27(3):249-62. doi:10.1016/j.devcel.2013.09.016.
Vitamin E Is Delivered to Cells via the High Affinity Receptor for Low-Density Lipoprotein. Traber MG, Kayden HJ. The American Journal of Clinical Nutrition. 1984;40(4):747-51. doi:10.1093/ajcn/40.4.747.
LDLs Stimulate P38 MAPKs and Wound Healing Through SR-BI Independently of Ras and PI3 Kinase. Bulat N, Waeber G, Widmann C. Journal of Lipid Research. 2009;50(1):81-9. doi:10.1194/jlr.M800119-JLR200.
The Interaction of Human Serum Components With Model Membranes Containing Phospholipids and Lipopolysaccharides. Paracini N, Correa Y, Del Giudice R, et al. Journal of Colloid and Interface Science. 2025;688:150-160. doi:10.1016/j.jcis.2025.02.131.
Inflammation, Aging, and Cardiovascular Disease: JACC Review Topic of the Week. Liberale L, Badimon L, Montecucco F, et al. Journal of the American College of Cardiology. 2022;79(8):837-847. doi:10.1016/j.jacc.2021.12.017.
Association Between Low Density Lipoprotein and All Cause and Cause Specific Mortality in Denmark: Prospective Cohort Study. Johannesen CDL, Langsted A, Mortensen MB, Nordestgaard BG. BMJ (Clinical Research Ed.). 2020;371:m4266. doi:10.1136/bmj.m4266.
Low-Density-Lipoprotein Cholesterol and Mortality Outcomes Among Healthy Older Adults: A Post Hoc Analysis of ASPREE Trial. Zhou Z, Tonkin AM, Curtis AJ, et al. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2024;79(4):glad268. doi:10.1093/gerona/glad268.
Lack of an Association or an Inverse Association Between Low-Density-Lipoprotein Cholesterol and Mortality in the Elderly: A Systematic Review. Ravnskov U, Diamond DM, Hama R, et al. BMJ Open. 2016;6(6):e010401. doi:10.1136/bmjopen-2015-010401.
Low and High-Density Lipoprotein Cholesterol and 10-Year Mortality in Community-Dwelling Older Adults: The Shanghai Aging Study. Wu W, Xiao Z, Liang X, et al. Frontiers in Medicine. 2022;9:783618. doi:10.3389/fmed.2022.783618.
Periodontitis and cardiometabolic disorders: The role of lipopolysaccharide and endotoxemia. Pussinen PJ, Kopra E, Pietiäinen M, et al. Periodontology 2000. 2022;89(1):19-40. doi:10.1111/prd.12433.
LPS-binding Protein Circulates in Association With apoB-containing Lipoproteins and Enhances Endotoxin-LDL/VLDL Interaction. Vreugdenhil AC, Snoek AM, van 't Veer C, Greve JW, Buurman WA. The Journal of Clinical Investigation. 2001;107(2):225-34. doi:10.1172/JCI10832.
Cholesterol, Inflammation and Innate Immunity. Tall AR, Yvan-Charvet L. Nature Reviews. Immunology. 2015;15(2):104-16. doi:10.1038/nri3793.
Question 2
Carroll MD et al.[1] Trends in Serum Lipids and Lipoproteins of Adults, 1960-2002. JAMA. 2005.
Balder JW et al.[2] Lipid and Lipoprotein Reference Values From 133,450 Dutch Lifelines Participants. J Clin Lipidol. 2017.
Feng L et al.[3] Age-Related Trends in Lipid Levels: A Large-Scale Cross-Sectional Study of the General Chinese Population. BMJ Open. 2020.
Zhang P et al.[4] Trends in LDL-C and Non-HDL-C Levels With Age. Aging Dis. 2020.
Martin SS et al.[5] Lipid Distributions in the Global Diagnostics Network Across Five Continents. Eur Heart J. 2023.
Ferrara A et al.[10] Total, LDL, and HDL Cholesterol Decrease With Age in Older Men and Women. The Rancho Bernardo Study 1984-1994. Circulation. 1997.
Kumar M et al.[6] Life's Essential 8: Optimizing Health in Older Adults. JACC Adv. 2023.
US Preventive Services Task Force.[7] Statin Use for the Primary Prevention of Cardiovascular Disease in Adults. JAMA. 2016.
Rozing MP, Westendorp RGJ.[8] Altered Cardiovascular Risk Pattern of LDL Cholesterol in Older Adults. Curr Opin Lipidol. 2023.
Bays HE et al.[9] National Lipid Association Annual Summary of Clinical Lipidology 2015. J Clin Lipidol. 2014.
van der Ploeg MA et al.[11] The Role of a Composite Fitness Score in the Association Between Low-Density Cholesterol and All-Cause Mortality in Older Adults. J Gerontol A Biol Sci Med Sci. 2023.
Ridker PM.[12] LDL Cholesterol: Controversies and Future Therapeutic Directions. Lancet. 2014.
Trinh MN et al.[13] Last Step in the Path of LDL Cholesterol From Lysosome to Plasma Membrane to ER Is Governed by Phosphatidylserine. Proc Natl Acad Sci USA. 2020.
Kanerva K et al.[14] LDL Cholesterol Recycles to the Plasma Membrane via a Rab8a-Myosin5b-Actin-Dependent Membrane Transport Route. Dev Cell. 2013.
Traber MG, Kayden HJ.[15] Vitamin E Is Delivered to Cells via the High Affinity Receptor for Low-Density Lipoprotein. Am J Clin Nutr. 1984.
Bulat N et al.[16] LDLs Stimulate P38 MAPKs and Wound Healing Through SR-BI Independently of Ras and PI3 Kinase. J Lipid Res. 2009.
Paracini N et al.[17] The Interaction of Human Serum Components With Model Membranes Containing Phospholipids and Lipopolysaccharides. J Colloid Interface Sci. 2025.
Liberale L et al.[18] Inflammation, Aging, and Cardiovascular Disease: JACC Review Topic of the Week. J Am Coll Cardiol. 2022.
Johannesen CDL et al.[19] Association Between Low Density Lipoprotein and All Cause and Cause Specific Mortality in Denmark: Prospective Cohort Study. BMJ. 2020.
Zhou Z et al.[20] Low-Density-Lipoprotein Cholesterol and Mortality Outcomes Among Healthy Older Adults: A Post Hoc Analysis of ASPREE Trial. J Gerontol A Biol Sci Med Sci. 2024.
Ravnskov U et al.[21] Lack of an Association or an Inverse Association Between Low-Density-Lipoprotein Cholesterol and Mortality in the Elderly: A Systematic Review. BMJ Open. 2016.
Wu W et al.[22] Low and High-Density Lipoprotein Cholesterol and 10-Year Mortality in Community-Dwelling Older Adults: The Shanghai Aging Study. Front Med (Lausanne). 2022.
Pussinen PJ et al.[23] Periodontitis and Cardiometabolic Disorders: The Role of Lipopolysaccharide and Endotoxemia. Periodontol 2000. 2022.
Vreugdenhil AC et al.[24] LPS-binding Protein Circulates in Association With apoB-containing Lipoproteins and Enhances Endotoxin-LDL/VLDL Interaction. J Clin Invest. 2001.
Tall AR, Yvan-Charvet L.[25] Cholesterol, Inflammation and Innate Immunity. Nat Rev Immunol. 2015.
Updates
Get low- and no-cost health tips and root-cause solutions.
FrugalDoc
Affordable Health & Wellness
© 2025 FrugalDoc Health & Wellness. All rights reserved.