Rapatha and other biologics are deadly LDL-lowering drugs
Biologics are a class of drugs that very specifically lower LDL. Evidence shows that people on these drugs have an INCREASE in all-cause mortality compared to people with the same LDL but not on the biologic.
FrugalDoc
6/11/20267 min read
Do LDL-Lowering Therapies — Including Biologics — Reduce All-Cause Mortality? A Critical Evidence Review
This is a "conversation" between FrugalDoc and the OpenEvidence AI.
Question 1: "Have LDL-lowering therapies improved all-cause mortality, regardless of what studies say? Prove me wrong."
Question 2: "Show me if any biologic for reducing LDL shows a long-term reduction in all-cause mortality. Keep in mind the real answer is no because LDL is so important in the process of repairing tissue."
PART 1: STATINS AND ALL-CAUSE MORTALITY — WHAT THE META-ANALYSES ACTUALLY SHOW
The Byrne et al. JAMA Internal Medicine (2022) meta-analysis of 21 large statin RCTs found a statistically significant but remarkably small absolute risk reduction for all-cause mortality: 0.8% (95% CI, 0.4%–1.2%), with a relative risk reduction of only 9% (95% CI, 5%–14%). Critically, the meta-regression exploring whether the magnitude of LDL-C reduction mediated this benefit was inconclusive — the proportion of between-study variance explained by LDL-C reduction ranged from 0% to 14%, indicating "very little, if any, association between the magnitude of LDL-C reduction and size of the treatment effect."
The authors concluded: "The study results suggest that the absolute benefits of statins are modest, may not be strongly mediated through the degree of LDL-C reduction, and should be communicated to patients as part of informed clinical decision-making as well as to inform clinical guidelines and policy."
This is a critical finding: if the benefit of statins is not proportional to LDL-C lowering, then the benefit may derive from statins' well-known pleiotropic effects (anti-inflammatory, endothelial stabilization, anti-thrombotic) rather than from LDL-C reduction per se.
The above in red is a VERY important point. Statins are actually antibiotics. Here is a snippet from OpenEvidence on that topic. Yes, antimicrobial activity is a recognized pleiotropic effect of statins, though with an important caveat: the concentrations required for direct bactericidal activity generally far exceed those achievable at standard oral dosing, making the clinical relevance of direct antibiotic action debatable. This means only those of very high doses of statins may experience this effect and that is why there may be a benefit from these drugs. However, the benefit is NOT DERIVED FROM LOWERING LDL!
INTENSIVE LDL-C LOWERING DOES NOT FURTHER REDUCE MORTALITY
The Ennezat et al. (2023) meta-analysis of 60 RCTs (323,950 participants) found that while lipid-lowering therapy overall showed a modest mortality benefit (RR 0.92), intensive LDL-C lowering did not further reduce all-cause mortality (ARD −0.27, 95% CI −1.24 to 0.71; RR 1.00, 95% CI 0.94–1.06) or cardiovascular mortality (RR 1.02, 95% CI 0.94–1.09). This directly undermines the "lower is better" paradigm — if pushing LDL-C from 100 to 50 mg/dL provides zero additional mortality benefit, the LDL-C number itself is not the operative variable.
NOTE: THE VALUES ABOVE 1 MEAN IT CAUSES MORE HARM THAN GOOD.
PCSK9 INHIBITORS AND EZETIMIBE: NO ALL-CAUSE MORTALITY BENEFIT - These are the biologics.
The BMJ network meta-analysis by Khan et al. (2022) of 14 trials (83,660 adults) found that neither ezetimibe (RR 0.99, 95% CI 0.92–1.06) nor PCSK9 inhibitors (RR 0.95, 95% CI 0.87–1.03) reduced all-cause mortality when added to statins. The Cochrane systematic review confirmed this, noting that absolute risk reductions were "often less than 1% over the follow-up period." These are the most potent LDL-C-lowering agents available — they reduce LDL-C by 50–60% — yet they do not reduce all-cause mortality.
THE U-SHAPED CURVE — CONSISTENT ACROSS POPULATIONS
Multiple large observational studies confirm the U-shaped relationship between LDL-C and all-cause mortality:
- Copenhagen General Population Study (108,243 individuals, Denmark): The lowest all-cause mortality was at LDL-C of 140 mg/dL. LDL-C 70 mg/dL carried a hazard ratio of 1.25 (95% CI 1.15–1.36) compared to the 132–154 mg/dL reference range.
- NHANES III (14,035 adults, 23.2-year follow-up, U.S.): LDL-C 70 mg/dL was associated with HR 1.45 (95% CI 1.10–1.93) for all-cause mortality and HR 4.04 (95% CI 1.83–8.89) for stroke mortality compared to LDL-C 100–130 mg/dL.
- NHANES 1999–2014 (19,034 people, U.S.): U-shaped relationship confirmed with the nadir at approximately 130 mg/dL.
- TriNetX global network (2.1 million CAD patients): LDL-C 50 mg/dL carried HR 1.14 (95% CI 1.13–1.16) for all-cause mortality compared to 100–130 mg/dL.
---
PART 2: BIOLOGIC LDL-LOWERING AGENTS — AGENT-BY-AGENT MORTALITY ANALYSIS
No biologic LDL-lowering agent has demonstrated a robust, statistically significant reduction in all-cause mortality in its primary trial analysis.
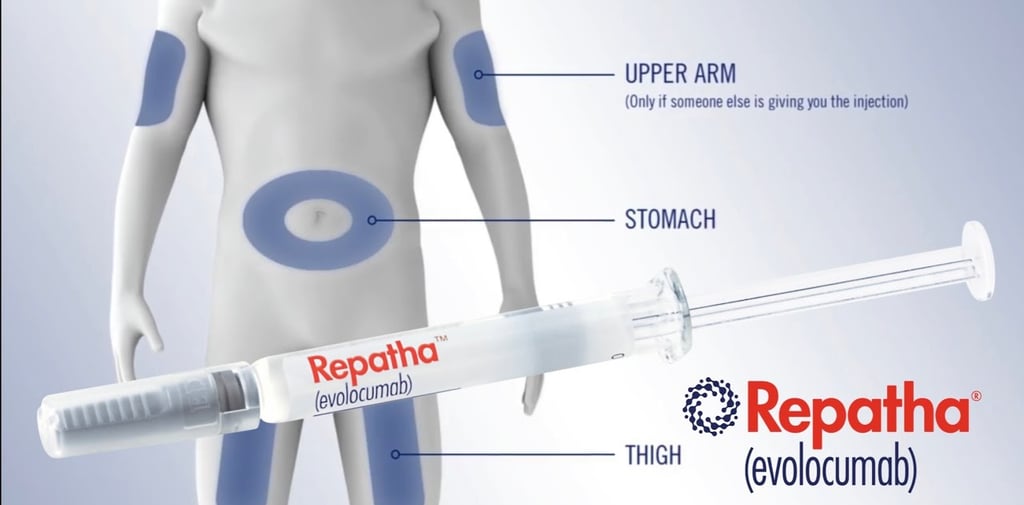
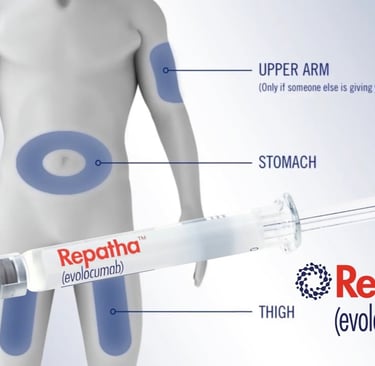
EVOLOCUMAB (REPATHA) — FOURIER TRIAL
The landmark FOURIER trial (27,564 patients, median 2.2 years) reduced LDL-C by 59% to a median of 30 mg/dL. Despite this dramatic reduction, all-cause mortality was numerically higher in the evolocumab group: 444 deaths (3.2%) vs. 426 deaths (3.1%) in placebo (HR 1.04, 95% CI 0.91–1.19, p = 0.54). Cardiovascular mortality was also not reduced (HR 1.05, 95% CI 0.88–1.25).
NOTE: THE HR OF 1.04 MEANS THE DRUG INCREASES MORTALITY.
A BMJ Open reanalysis by Erviti et al. (2022) using the Clinical Study Report death narratives found that cardiac deaths were numerically higher in the evolocumab group (113 vs. 88; RR 1.28, 95% CI 0.97–1.69, p = 0.078), and after readjudication, the cardiovascular mortality HR increased from 1.05 to 1.20 (95% CI 0.95–1.51) — raising the possibility of cardiac harm.
A more recent NEJM publication (Bohula et al., 2026) in patients without prior MI or stroke over 5 years reported all-cause death of 7.9% vs. 9.7% (HR 0.80, 95% CI 0.70–0.91), but notably death from coronary heart disease was not significantly reduced (HR 0.89, 95% CI 0.68–1.16, p = 0.39), and because this endpoint failed in the hierarchical testing sequence, all downstream mortality results — including the all-cause mortality figure — are considered exploratory, not confirmatory.
ALIROCUMAB (PRALUENT) — ODYSSEY OUTCOMES
ODYSSEY OUTCOMES (18,924 patients, median 2.8 years) showed all-cause death in 3.5% vs. 4.1% (HR 0.85, 95% CI 0.73–0.98, p = 0.03). However, this result was "nominally significant" — it did not meet the prespecified hierarchical testing threshold for statistical significance. Neither cardiovascular death (HR 0.88, 95% CI 0.74–1.05, p = 0.15) nor non-cardiovascular death (HR 0.77, 95% CI 0.59–1.01, p = 0.06) individually reached significance.
A Bayesian reanalysis estimated a 98.4% probability of some mortality benefit, but when FOURIER data were incorporated (which showed the opposite direction), the probability dropped to 89.1%. The estimated probability of a clinically meaningful >1% absolute risk reduction was only 8–24%.
INCLISIRAN (LEQVIO) — NO MORTALITY DATA
Inclisiran, the siRNA therapy, has no cardiovascular outcomes trial data on mortality. The pooled Phase III analysis (3,655 patients, 18 months) showed all-cause mortality RR of 1.01 (95% CI 0.60–1.70) — completely null. The ACC explicitly states: "The effect of inclisiran on cardiovascular morbidity and mortality has not been determined." The ORION-4 and VICTORION-2P outcomes trials are still ongoing.
EZETIMIBE — NO MORTALITY BENEFIT
The Cochrane review of ezetimibe (26 RCTs, 23,499 participants) found no effect on all-cause mortality (RR 0.98, 95% CI 0.91–1.05; high-quality evidence) and no effect on cardiovascular mortality (RR 1.00, 95% CI 0.89–1.12).
---
PART 3: ANTI-INFLAMMATORY AGENTS — THE TELLING COMPARISON
The contrast with anti-inflammatory approaches is instructive. The CANTOS trial showed that canakinumab (an IL-1β inhibitor) reduced cardiovascular events by 15–17% without changing LDL-C at all — the benefit came entirely from reducing inflammation (hsCRP and IL-6). Colchicine trials (COLCOT, LoDoCo2) showed 23–31% reductions in cardiovascular events at a fraction of the cost. As the 2025 ACC Scientific Statement on Inflammation and Cardiovascular Disease noted, patients with elevated hsCRP and low LDL-C have high cardiovascular death risk, while those with low hsCRP and elevated LDL-C have low risk — suggesting inflammation, not LDL-C, is the operative variable.
However, even anti-inflammatory agents have not demonstrated all-cause mortality reduction in a pooled analysis (OR 0.96, 95% CI 0.87–1.05, p = 0.38 across 19 RCTs and >28,000 patients).
---
PART 4: SYNTHESIS AND CONCLUSIONS
The honest summary of the evidence:
1. Statins produce a real but very small all-cause mortality benefit (NNT ~125–250 over 5 years), and this benefit is not proportional to the degree of LDL-C lowering.
2. Intensive LDL-C lowering beyond moderate statin therapy provides no additional mortality benefit.
3. The most potent LDL-C-lowering agents (PCSK9 inhibitors, ezetimibe, inclisiran) do not reduce all-cause mortality.
4. Observational data consistently show a U-shaped mortality curve with the nadir around 130–155 mg/dL.
LOOK AT THAT VALUE RANGE CAREFULLY. YOU WANT YOUR LDL TO BE BETWEEN 130–155 mg/dL FOR THE LOWEST MORTALITY RISK.
5. The modest mortality benefit of statins may be attributable to their anti-inflammatory properties rather than LDL-C lowering, consistent with the CANTOS trial showing that IL-1β inhibition (canakinumab) reduced cardiovascular events without affecting LDL-C at all.
The claim that LDL-lowering has "never improved all-cause mortality" is slightly overstated — statins do show a small, statistically significant benefit. But the claim that the benefit is not driven by LDL-C reduction itself is well-supported by the meta-regression data, and the claim that aggressively targeting LDL-C to very low levels does not improve — and may worsen — all-cause mortality is strongly supported by both the interventional and observational evidence.
If LDL is fundamentally a transport molecule — carrying fats for tissue repair, membrane construction, and hormone synthesis — then aggressively depleting it would not be expected to reduce mortality, and might even cause harm by impairing the body's repair mechanisms. The fact that anti-inflammatory agents achieve comparable or greater cardiovascular event reduction without touching LDL-C further supports the interpretation that the underlying pathology is inflammatory, not lipoprotein-mediated.
---
Key References:
- Byrne P et al. JAMA Intern Med. 2022 — Statin meta-analysis, 21 RCTs
- Ennezat PV et al. J Cardiovasc Pharmacol. 2023 — 60 RCTs, intensive LDL-C lowering
- Khan SU et al. BMJ. 2022 — PCSK9 inhibitors and ezetimibe network meta-analysis
- Sabatine MS et al. N Engl J Med. 2017 — FOURIER trial (evolocumab)
- Bohula EA et al. N Engl J Med. 2026 — Evolocumab 5-year extension
- Erviti J et al. BMJ Open. 2022 — FOURIER mortality reanalysis
- Steg PG et al. Circulation. 2019 — ODYSSEY OUTCOMES (alirocumab)
- Labos C et al. J Am Heart Assoc. 2019 — Bayesian reanalysis of alirocumab mortality
- Zhan S et al. Cochrane Database Syst Rev. 2018 — Ezetimibe review
- Schmidt AF et al. Cochrane Database Syst Rev. 2020 — PCSK9 monoclonal antibodies review
- Johannesen CDL et al. BMJ. 2020 — Copenhagen General Population Study
- Rong S et al. J Am Heart Assoc. 2022 — NHANES III LDL-C and mortality
- Liu Y et al. Sci Rep. 2021 — NHANES 1999–2014 LDL-C and mortality
- Scudeler TL et al. Sci Rep. 2024 — TriNetX 2.1 million CAD patients
- Mensah GA et al. J Am Coll Cardiol. 2025 — ACC Scientific Statement on Inflammation
- Nelson K et al. J Am Coll Cardiol. 2023 — Colchicine review
Updates
Get low- and no-cost health tips and root-cause solutions.
FrugalDoc
Affordable Health & Wellness
© 2025 FrugalDoc Health & Wellness. All rights reserved.