More on Why Lowering LDL With Statins or Biologics is WRONG
The evidence strongly suggests that much of the MEAGER mortality benefit in a very specific group only, attributed to statins comes from their pleiotropic effects — anti-inflammatory, immunomodulatory, and antimicrobial — rather than from LDL lowering
FrugalDoc
7/3/202611 min read
LDL lowering is NOT why statin drugs provide meager benefit in those with severe cardiovascular disease, despite what you are told.
This is yet another in a series of blogs on LDL-lowering, statins, and biologics prescriptions. Why? Because almost all traditional doctors don't know how to address your health issues. So, it is safe for them to prescribe statins, and they do so for symptoms and conditions that they have NEVER been proven to help. Why do doctors do this? Because almost everyone has a "high" LDL level based on the current standard-of-care reference range - which is completely wrong, as cited in other blogs. If you see your doctor and they did something, they are safe from liability. My mentor at Harvard Medical School made the point that prescribing statins is a "religion" in the standard-of-care of medicine.
OpenEvidence Answer:
This is a critically important question that the data answer quite clearly. The evidence strongly suggests that much of the mortality benefit attributed to statins comes from their pleiotropic effects — anti-inflammatory, immunomodulatory, and antimicrobial — rather than from LDL lowering per se, and the PCSK9 inhibitor data serve as a natural experiment that helps disentangle these contributions.
The PCSK9 Inhibitor "Natural Experiment"
PCSK9 inhibitors like evolocumab (Repatha) are essentially pure LDL-lowering agents — they reduce LDL-C by ~60% without the pleiotropic effects of statins.[1] This makes them an ideal comparator for isolating the contribution of LDL lowering alone:
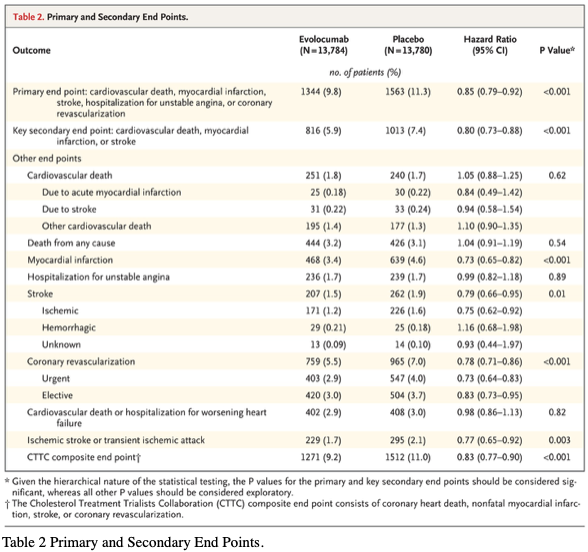
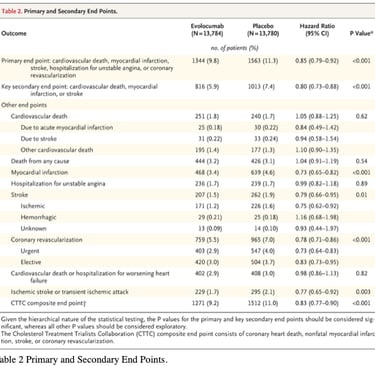
- FOURIER trial (evolocumab, n=27,564, median 2.2 years): Despite reducing LDL-C by 59%, evolocumab showed no reduction in cardiovascular death (HR 1.05; 95% CI 0.88–1.25) and no reduction in all-cause mortality (HR 1.04; 95% CI 0.91–1.19). This is the HR of 1.04 referenced in the question.[2][3]
- ODYSSEY OUTCOMES (alirocumab, n=18,924, median 2.8 years): Showed a borderline reduction in all-cause mortality (HR 0.85; 95% CI 0.73–0.98) but no significant reduction in cardiovascular mortality (HR 0.88; 95% CI 0.74–1.05).[3]
- A Cochrane meta-analysis of PCSK9 inhibitor trials confirmed that while MACE was reduced, there was no significant difference in cardiovascular mortality (OR 0.94; 95% CI 0.83–1.07).[4]
The FOURIER data from the original trial are shown in the following table:
This is another blog generated by having a conversation with Harvard's and MIT's medical AI, OpenEvidence.
FrugalDoc Question / Comment:
In a previous conversation on LDL lowering, you presented data on biologics to reduce LDL that showed an overall hazard ratio for early all-cause mortality of 1.04. We also established that, for people over 60, lowering LDL increases mortality. This was published in the Mayo Clinic Proceedings as "Atherogenic Index of Plasma and Triglyceride/High-Density Lipoprotein Cholesterol Ratio Predict Mortality Risk Better Than Individual Cholesterol Risk Factors Among an Older Adult Population." The biologics work in one way: by lowering LDL production. Statins are pleiotropic. They lower LDL, CoQ10, and the evidence that they are antimicrobial is strong. https://academic.oup.com/jac/article-pdf/61/2/362/2307058/dkm496.pdf Unexpected antimicrobial effect of statins. That being the case, what can you conclude about LDL-lowering and health benefits, including longevity, compared with other effects of statin drugs that do not occur with biologics like Repatha?
Implication:
Statins are the WRONG drug. The actual reason for their action suggests the need for better and safer treatments.
Statins lower CQ10 - This is very bad!
ATP, your energy molecule, is made in the mitochondria through a 4-step process. Coenzyme Q10 acts as the vital, mobile link that bridges the first two complexes to the third.
Key Conclusion:
The fact that statins reduce mortality equally in non-cardiovascular conditions as in cardiovascular disease is a striking finding that cannot be explained by LDL lowering.
The fact that statins reduce mortality equally in non-cardiovascular conditions as in cardiovascular disease is a striking finding that cannot be explained by LDL lowering.
What Statins Do That Biologics Do Not
The following pleiotropic mechanisms are unique to statins and absent from PCSK9 inhibitors:
1. Anti-inflammatory effects. Statins reduce CRP by 37% (JUPITER trial), IL-6, TNF-α, and NF-κB activation through mevalonate pathway inhibition — effects that are independent of LDL lowering.[7][8][9] Ezetimibe, which lowers LDL without inhibiting HMG-CoA reductase, does not reduce CRP unless combined with a statin.[10] The JUPITER trial demonstrated a 47% reduction in cardiovascular events in patients with normal LDL but elevated CRP — a population where LDL lowering alone would not be expected to help.[8] The 2025 ACC Scientific Statement on Inflammation and Cardiovascular Disease explicitly recognizes that reductions in both LDL and hsCRP contribute to statin benefit.[8]
2. Antimicrobial effects — directly relevant to atherosclerosis. Statins directly inhibit the growth of Chlamydophila pneumoniae — the very organism implicated in atherosclerotic plaque inflammation.[12][13] Specifically:
- Atorvastatin and lovastatin reduce in vitro growth of C. pneumoniae[12]
- Cerivastatin reduced C. pneumoniae transmission from macrophages to vascular smooth muscle cells by 33%, blocked RhoA/Rac1 prenylation, suppressed NF-κB activation, and inhibited RANTES and MCP-1 chemokine production in infected cells[13]
- Simvastatin reduced C. pneumoniae-mediated histone modifications and inflammatory gene expression in endothelial cells via Rac1 inhibition[14]
- Statins also show antiviral effects against CMV, EBV, hepatitis C, dengue, and HIV — all through mevalonate pathway inhibition rather than cholesterol lowering[12][15]
This is particularly significant given the infectious hypothesis of atherosclerosis. If a substantial component of atherosclerotic plaque inflammation is driven by intracellular pathogens like C. pneumoniae, then statins would address this through their antimicrobial properties while PCSK9 inhibitors would not.
3. Endothelial function improvement. Statins induce endothelial nitric oxide synthase (eNOS), increasing NO production and causing vascular relaxation — demonstrated in animals even when cholesterol levels were held constant.[10]
4. CoQ10 depletion — a double-edged sword. Statins reduce CoQ10 synthesis as a collateral effect of mevalonate pathway inhibition.[16] While this causes the well-known muscle symptoms in some patients, CoQ10 depletion may paradoxically contribute to some of the pleiotropic effects by altering mitochondrial signaling. The 2018 ACC/AHA guidelines note that available evidence does not support routine CoQ10 supplementation for SAMS.[17]
The LDL Paradox in Older Adults
The data on LDL and mortality in older adults add another dimension to this analysis:
- A systematic review of 19 cohort studies (68,094 elderly individuals) found that high LDL-C was inversely associated with all-cause mortality in 92% of cohorts where this was examined — meaning higher LDL was associated with living longer.[18]
- The ASPREE post-hoc analysis (12,334 adults ≥65 years, 7-year follow-up) found a U-shaped relationship: per 1 mmol/L higher LDL-C, all-cause mortality decreased by 9%, cancer mortality by 16%, and non-CVD/non-cancer mortality by 18% — while CVD mortality increased by 19%.[19]
- An individual patient data meta-analysis of very old adults (median age 85) found an inverse association between LDL-C and 5-year mortality (HR 0.87 per 1 mmol/L increase), most pronounced in those with low fitness scores.[20]
- A NHANES analysis (19,034 participants) confirmed a U-shaped relationship between LDL-C and all-cause mortality, with the lowest LDL group having 37% higher mortality than the reference group.[21]
- A recent UK Biobank study found that the TG/HDL-C ratio (atherogenic index) predicted ASCVD risk in younger adults, but this association steadily attenuated with age — in adults over 65, an elevated ratio may even be associated with lower ASCVD risk.[22]
A recent JACC Advances study illustrates the concept of a "Goldilocks zone" for lipid levels in older adults, showing that both very low and very high LDL-C levels increase cardiovascular risk:
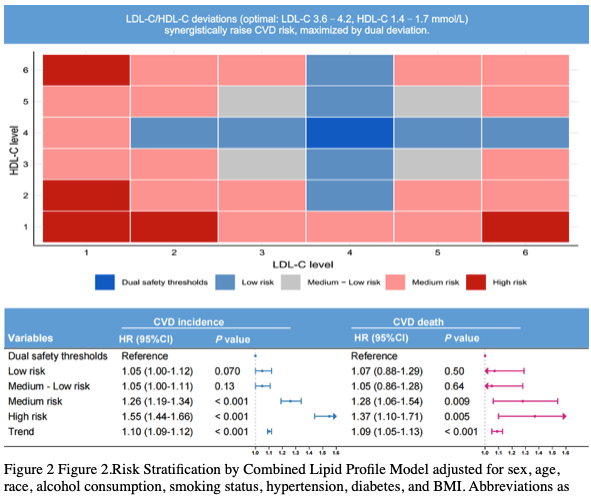
What this chart says:
Column 1: VERY low LDL (favored by your doctor) - very high risk.
Column 2: low LDL - high risk
Column 3: Lowish LDL (IMHO) but on the high end of your doctor's good level: still unacceptable risk. Why isn't it no risk if your doctor likes this level?
Column 4: High end of normal and "too high" per your regular doctor: Lowest risk
Column 5: Ouch, your doctor would say you need a statin "now." Yet this carries much lower risk than column 2, where your doctor would be very happy with your LDL!
Column 6: Very high LDL (>230). This has high risk, but as you read this blog, it is because the LDL is RESPONDING to something. It is not the reason for the high risk.
Note: The best outcomes, shown in column 4, are at LDL levels of 3.5 to 4.5 mmol/L. This translates to 135-175 mg/dL, the units used in the U.S.
Synthesis: What Can Be Concluded
The convergence of these data points supports several conclusions:
1. LDL lowering alone is insufficient to reduce mortality. PCSK9 inhibitors achieve dramatic LDL reductions (~60%) but have failed to demonstrate consistent all-cause or cardiovascular mortality reduction across trials, with the FOURIER HR of 1.04 for all-cause mortality being the starkest example.[2][26][3]
FrugalDoc: That is a generous conclusion considering that the super LDL lowering drugs like Repatha INCREASE MORTALITY.
2. Statins reduce mortality through mechanisms INDEPENDENT OF LDL lowering. The mortality benefit of statins in both CVD and non-CVD populations (HR 0.72 in DRUG COMPANY SPONSORED data) is primarily due to their anti-inflammatory/antimicrobial properties, collectively indicating that the pleiotropic effects are clinically meaningful.[6][8][9]
3. The antimicrobial effect may be underappreciated. Statins directly suppress C. pneumoniae growth and its inflammatory activation of vascular cells — an effect that PCSK9 inhibitors cannot replicate. If chronic intracellular infection contributes to atherosclerotic inflammation (as the infectious hypothesis proposes), this antimicrobial property could account for a meaningful portion of statin benefit.[13][14][27]
4. In older adults, the risk-benefit calculus shifts. The observational data showing inverse LDL-mortality associations in the elderly, combined with the failure of pure LDL-lowering biologics to reduce mortality, suggest that aggressively lowering LDL in older adults may remove a substance that serves protective functions (immune defense, membrane integrity, hormone synthesis) while failing to address the inflammatory and infectious drivers of atherosclerosis.[19][20][18]
5. The most logical interpretation is that statins are effective not because they lower LDL, but because they are anti-inflammatory, immunomodulatory, and antimicrobial agents that happen to also lower LDL. LDL-lowering may reduce atherosclerotic events (particularly MI and stroke), but the mortality benefit appears to derive predominantly from non-LDL effects. This interpretation is consistent with the observation that other non-statin LDL-lowering agents (ezetimibe, PCSK9 inhibitors) have weaker, absent, or adverse mortality signals.
Would you like to explore the CANTOS trial data (canakinumab, a pure anti-inflammatory IL-1β inhibitor) and how its cardiovascular outcomes further support the hypothesis that inflammation — rather than LDL — is the primary driver of atherosclerotic mortality?
THIS IMPORTANT RESULT WILL BE THE SUBJECT OF THE NEXT BLOG. STAY TUNED.
References
Proprotein Convertase Subtilisn/Kexin Type 9 Inhibitors and Small Interfering RNA Therapy for Cardiovascular Risk Reduction: A Systematic Review and Meta-Analysis. Imran TF, Khan AA, Has P, et al. PloS One. 2023;18(12):e0295359. doi:10.1371/journal.pone.0295359.
Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. Sabatine MS, Giugliano RP, Keech AC, et al. The New England Journal of Medicine. 2017;376(18):1713-1722. doi:10.1056/NEJMoa1615664.
Low LDL Cholesterol by PCSK9 Variation Reduces Cardiovascular Mortality. Benn M, Tybjærg-Hansen A, Nordestgaard BG. Journal of the American College of Cardiology. 2019;73(24):3102-3114. doi:10.1016/j.jacc.2019.03.517.
PCSK9 Monoclonal Antibodies for the Primary and Secondary Prevention of Cardiovascular Disease. Schmidt AF, Carter JL, Pearce LS, et al. The Cochrane Database of Systematic Reviews. 2020;10:CD011748. doi:10.1002/14651858.CD011748.pub3.
Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. Chou R, Cantor A, Dana T, et al. JAMA. 2022;328(8):754-771. doi:10.1001/jama.2022.12138.
Effect of Statins on All-Cause Mortality in Adults: A Systematic Review and Meta-Analysis of Propensity Score-Matched Studies. Nowak MM, Niemczyk M, Florczyk M, Kurzyna M, Pączek L. Journal of Clinical Medicine. 2022;11(19):5643. doi:10.3390/jcm11195643.
Impact of Statins as Immune-Modulatory Agents on Inflammatory Markers in Adults With Chronic Diseases: A Systematic Review and Meta-Analysis. Sabeel S, Motaung B, Nguyen KA, et al. PloS One. 2025;20(5):e0323749. doi:10.1371/journal.pone.0323749.
Inflammation and Cardiovascular Disease: 2025 ACC Scientific Statement: A Report of the American College of Cardiology. Mensah GA, Arnold N, Prabhu SD, Ridker PM, Welty FK. Journal of the American College of Cardiology. 2025;:S0735-1097(25)07555-2. doi:10.1016/j.jacc.2025.08.047.
Innate and Adaptive Inflammation as a Therapeutic Target in Vascular Disease: The Emerging Role of Statins. Tousoulis D, Psarros C, Demosthenous M, et al. Journal of the American College of Cardiology. 2014;63(23):2491-2502. doi:10.1016/j.jacc.2014.01.054.
Targeting the Immune System in Atherosclerosis: JACC State-of-the-Art Review. Zhao TX, Mallat Z. Journal of the American College of Cardiology. 2019;73(13):1691-1706. doi:10.1016/j.jacc.2018.12.083.
Contribution of Statins towards Periodontal Treatment: A Review. Petit C, Batool F, Bugueno IM, et al. Mediators of Inflammation. 2019;2019:6367402. doi:10.1155/2019/6367402.
Potential Effect of Statins on Mycobacterium tuberculosis Infection. Guerra-De-Blas PDC, Torres-González P, Bobadilla-Del-Valle M, et al. Journal of Immunology Research. 2018;2018:7617023. doi:10.1155/2018/7617023.
Hydroxymethylglutaryl Coenzyme a Reductase Inhibition Reduces Chlamydia Pneumoniae-Induced Cell Interaction and Activation. Dechend R, Gieffers J, Dietz R, et al. Circulation. 2003;108(3):261-5. doi:10.1161/01.CIR.0000083367.93022.78.
Simvastatin Reduces Chlamydophila Pneumoniae-Mediated Histone Modifications and Gene Expression in Cultured Human Endothelial Cells. Schmeck B, Beermann W, N'Guessan PD, et al. Circulation Research. 2008;102(8):888-95. doi:10.1161/CIRCRESAHA.107.161307.
Statins: A Viable Candidate for Host-Directed Therapy Against Infectious Diseases. Parihar SP, Guler R, Brombacher F. Nature Reviews. Immunology. 2019;19(2):104-117. doi:10.1038/s41577-018-0094-3.
Coenzyme Q for Patients With Cardiovascular Disease: JACC Focus Seminar. Raizner AE, Quiñones MA. Journal of the American College of Cardiology. 2021;77(5):609-619. doi:10.1016/j.jacc.2020.12.009.
2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Grundy SM, Stone NJ, Bailey AL, et al. Journal of the American College of Cardiology. 2019;73(24):e285-e350. doi:10.1016/j.jacc.2018.11.003.
Lack of an Association or an Inverse Association Between Low-Density-Lipoprotein Cholesterol and Mortality in the Elderly: A Systematic Review. Ravnskov U, Diamond DM, Hama R, et al. BMJ Open. 2016;6(6):e010401. doi:10.1136/bmjopen-2015-010401.
Low-Density-Lipoprotein Cholesterol and Mortality Outcomes Among Healthy Older Adults: A Post Hoc Analysis of ASPREE Trial. Zhou Z, Tonkin AM, Curtis AJ, et al. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2024;79(4):glad268. doi:10.1093/gerona/glad268.
The Role of a Composite Fitness Score in the Association Between Low-Density Cholesterol and All-Cause Mortality in Older Adults: An Individual Patient Data Meta-Analysis. van der Ploeg MA, Poortvliet RKE, Bogaerts JMK, et al. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2023;78(9):1708-1716. doi:10.1093/gerona/glad148.
Association Between Low Density Lipoprotein Cholesterol and All-Cause Mortality: Results From the NHANES 1999-2014. Liu Y, Liu F, Zhang L, et al. Scientific Reports. 2021;11(1):22111. doi:10.1038/s41598-021-01738-w.
Advancing Age and Risk From the Elevated Atherogenic Index: Triglyceride (TG) to High-Density Cholesterol (HDL-C) Ratio. Kumar M, Zhao S, Robinson P, et al. Journal of the American Geriatrics Society. 2025;. doi:10.1111/jgs.19607.
U-Shaped Lipid-CVD Links in Older Adults: Reversed LDL-C and HDL-C Associations and Goldilocks Zone. Ye X, Du S, Chen S, et al. JACC. Advances. 2026;5(2):102544. doi:10.1016/j.jacadv.2025.102544.
Efficacy and Safety of Lowering LDL Cholesterol in Older Patients: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Gencer B, Marston NA, Im K, et al. Lancet (London, England). 2020;396(10263):1637-1643. doi:10.1016/S0140-6736(20)32332-1.
2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Writing Committee Members, Blumenthal RS, Morris PB, et al. Circulation. 2026;. doi:10.1161/CIR.0000000000001423.
Cardiovascular Events With PCSK9 Inhibitors: An Updated Meta-Analysis of Randomised Controlled Trials. Casula M, Olmastroni E, Boccalari MT, et al. Pharmacological Research. 2019;143:143-150. doi:10.1016/j.phrs.2019.03.021.
Hydroxymethylglutaryl Coenzyme a Reductase Inhibitors Modify the Inflammatory Response of Human Macrophages and Endothelial Cells Infected With Chlamydia Pneumoniae. Kothe H, Dalhoff K, Rupp J, et al. Circulation. 2000;101(15):1760-3. doi:10.1161/01.cir.101.15.1760.
Updates
Get low- and no-cost health tips and root-cause solutions.
FrugalDoc
Affordable Health & Wellness
© 2025 FrugalDoc Health & Wellness. All rights reserved.