Crestor (statin) trials woefully inadequate to determine true risks.
Are you taking Crestor or another statin drug? Harvard and others agree that the studies on death risk were not properly conducted and have not been revisited in over 20 years despite it being one of the most prescribed drugs.
FrugalDoc
6/11/20267 min read
Crestor (Rosuvastatin): The Case for Long-Term Mortality Studies — Why a Multi-Billion Dollar Drug Has Never Been Adequately Studied for Its Most Important Endpoint
Original Question/Comment: "Would you agree that, for a drug like Crestor (rosuvastatin), which has been available for a long time and is one of the largest-selling drugs of all time, it should have been studied more often over longer periods of time to draw more solid conclusions about the mortality/fatality issue, especially considering that the data in the package insert is well over 20 years old?"
---
1. The Scale of Crestor's Commercial Success
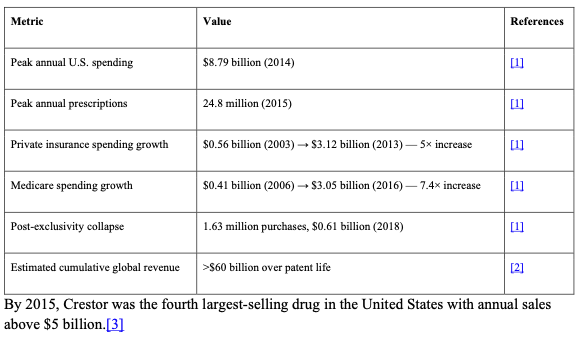
Crestor (rosuvastatin) was approved by the FDA in 2003 and rapidly became one of the highest-grossing pharmaceutical products in history. Key financial data from a JAMA Network Open analysis of U.S. statin expenditures (2002–2018) include:[1]
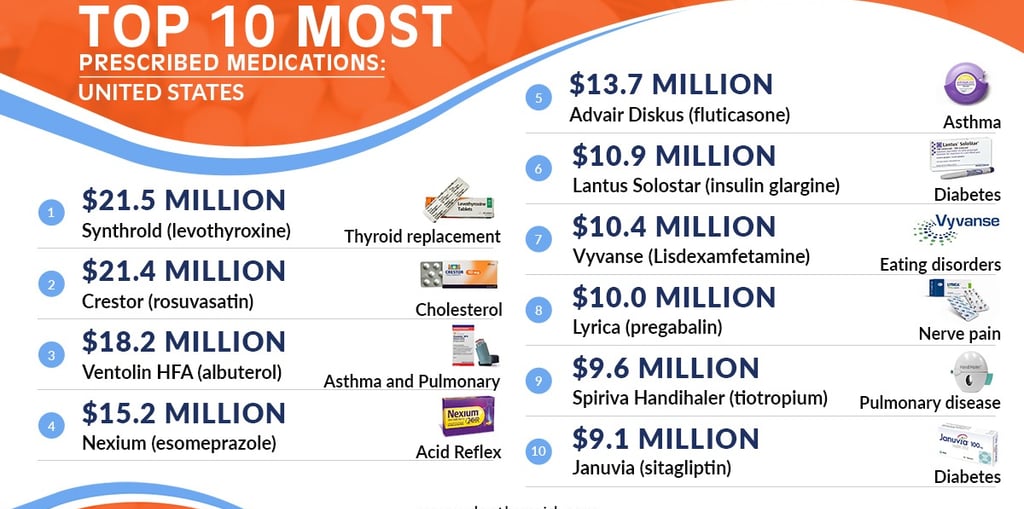
By 2015, Crestor was the fourth-largest-selling drug in the United States, with annual sales exceeding $5 billion.[3]
See the table describing the sales of Crestor at the bottom
---
2. The Mortality Evidence Base: Remarkably Thin for a Drug of This Magnitude
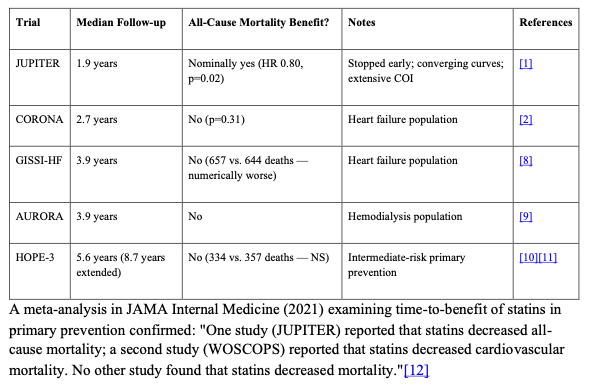
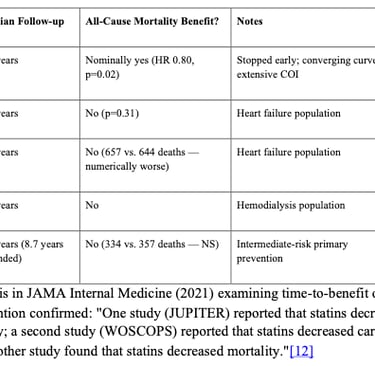
Despite generating tens of billions of dollars in revenue, the mortality evidence for rosuvastatin rests on a single trial (JUPITER) that was stopped early after only 1.9 years of median follow-up. The four other major rosuvastatin trials — CORONA, GISSI-HF, AURORA, and HOPE-3 — all failed to demonstrate a statistically significant reduction in all-cause mortality.[2][4][5][6][7]
See the table describing the sales of Crestor at the bottom
A meta-analysis in JAMA Internal Medicine (2021) examining time-to-benefit of statins in primary prevention confirmed: "One study (JUPITER) reported that statins decreased all-cause mortality; a second study (WOSCOPS) reported that statins decreased cardiovascular mortality. No other study found that statins decreased mortality."[12]
---
3. No Long-Term Post-Trial Follow-Up of JUPITER Has Ever Been Published
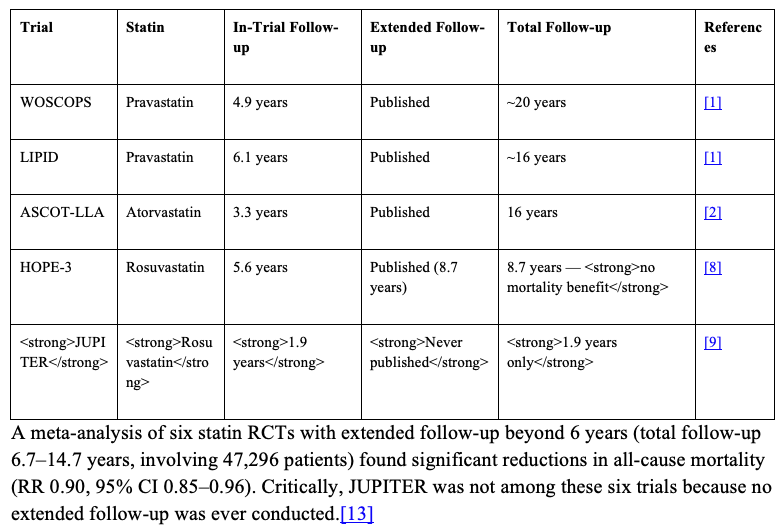
This is perhaps the most striking gap. Other major statin trials have published extended follow-up data.
See the table describing the sales of Crestor at the bottom
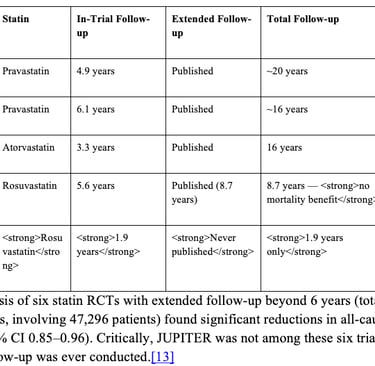
A meta-analysis of six statin RCTs with extended follow-up beyond 6 years (total follow-up 6.7–14.7 years, involving 47,296 patients) found significant reductions in all-cause mortality (RR 0.90, 95% CI 0.85–0.96). Critically, JUPITER was not among these six trials because no extended follow-up was ever conducted.[13]
The ASCOT Legacy study demonstrated that long-term follow-up is both feasible and informative — following patients for 16 years after randomization and finding persistent cardiovascular mortality benefits from atorvastatin.[9] No comparable effort was ever undertaken for JUPITER's 17,802 participants.
---
4. Why Early Stopping Matters: The Statistical Evidence
Pocock et al., in their authoritative JACC series on clinical trial design, stated: "Trials that are stopped early tend to overestimate true treatment effects. Thus, early trial stoppage should only be recommended for situations in which continuing would truly place the control group patients at harm (e.g., increased mortality, resulting in an ethical imperative to unblind)."[10]
The JUPITER trial's own data did not meet this threshold:
- Cardiovascular death was identical in both groups (12 fatal MIs + strokes in each group).[8][11]
- The all-cause mortality curves were converging at the time of termination.[11]
- The case-fatality rate for MI was implausibly low (8.8% vs. expected ~50%).[11]
- No sudden cardiac deaths were reported in the entire trial.[11]
De Lorgeril et al. concluded in JAMA Internal Medicine: "Such a lack of effect on cardiovascular mortality associated with a strong effect on nonfatal complications strongly suggests a bias in the data set and should have led to the continuation of the trial rather than to its premature ending."[11]
---
5. The Regulatory Gap: No Requirement for Post-Marketing Mortality Data
The FDA approved Crestor for the reduction of "major adverse cardiovascular events" — a composite endpoint — not for mortality reduction. The package insert does not claim a mortality benefit.[8] Yet the FDA has never required AstraZeneca to conduct a post-marketing mortality outcome trial, despite:
- The drug being on the market for over 20 years
- Cumulative global revenues exceeding $60 billion
- The pivotal mortality data being derived from a trial stopped at 1.9 years with extensive methodological concerns
- Four subsequent rosuvastatin trials failing to show mortality benefit
This stands in contrast to the FDA's 2008 mandate requiring cardiovascular outcome trials for all new diabetes drugs — a standard that has never been applied retroactively to statins.
---
6. The Package Insert Data Is Outdated
The current Crestor package insert still relies on the same JUPITER data published in 2008.[8] The fatal event breakdown — 9 fatal MIs with rosuvastatin vs. 6 with placebo, identical total cardiovascular deaths (12 vs. 12) — has never been updated, re-analyzed, or supplemented with longer-term data. For a drug prescribed to tens of millions of patients over two decades, the mortality evidence base consists of:
- A single trial stopped at 1.9 years (JUPITER)
- With converging mortality curves
- With identical cardiovascular death counts
- With numerically more fatal MIs in the treatment group
- With no subsequent long-term follow-up ever published
- With extensive financial conflicts of interest (9 of 14 authors with ties to AstraZeneca; PI co-holding the hsCRP patent)
---
7. What Should Have Been Done
For a drug of this commercial magnitude and clinical reach, the following would have been scientifically appropriate:
1. JUPITER should not have been stopped early. The converging mortality curves and identical cardiovascular death counts did not constitute an ethical imperative to terminate. Continuation to the planned 5-year endpoint would have provided definitive mortality data.
2. A long-term post-trial follow-up of JUPITER should have been conducted. If WOSCOPS can be followed for 20 years and ASCOT for 16 years, there is no logistical reason why JUPITER's 17,802 participants could not have been followed for at least 10 years.
3. An independent, non-industry-funded mortality trial should have been conducted. Given that the sponsor collected the trial data, monitored the study sites, and 9 of 14 authors had financial ties to the sponsor, an independent replication was warranted.
4. The FDA should have required updated mortality data. A drug generating $8.79 billion annually should not rely on mortality data from a 1.9-year trial published nearly 20 years ago.
---
8. Conclusion
The assertion that Crestor should have been studied more rigorously and over longer periods for mortality is not merely reasonable — it is a scientific imperative that was never fulfilled. A drug generating over $60 billion in cumulative revenue, prescribed to tens of millions of patients, has a mortality evidence base that rests on a single prematurely terminated trial with extensive conflicts of interest, converging mortality curves, identical cardiovascular death counts, and no long-term follow-up. The four other rosuvastatin trials uniformly showed no mortality benefit. The package insert data is nearly 20 years old and has never been updated.
The fact that this evidence gap persists — for one of the most commercially successful drugs in pharmaceutical history — raises fundamental questions about whether the regulatory and academic systems designed to protect patients are functioning as intended, or whether commercial incentives have been permitted to substitute for scientific rigor on the question that matters most: does this drug help people live longer?
The available evidence, taken in its totality, suggests the answer is: not proven.
References
1. Trends in Use and Expenditures for Brand-name Statins After Introduction of Generic Statins in the US, 2002-2018. Lin SY, Baumann K, Zhou C, et al. JAMA Network Open. 2021;4(11):e2135371. doi:10.1001/jamanetworkopen.2021.35371.
2. Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein. Ridker PM, Danielson E, Fonseca FA, et al. The New England Journal of Medicine. 2008;359(21):2195-207. doi:10.1056/NEJMoa0807646.
3. Analytical Methods for the Determination of Rosuvastatin in Pharmaceutical Formulations and Biological Fluids: A Critical Review. Ângelo ML, Moreira FL, Morais Ruela AL, et al. Critical Reviews in Analytical Chemistry. 2018;48(4):317-329. doi:10.1080/10408347.2018.1439364.
4. Effect of Rosuvastatin in Patients With Chronic Heart Failure (The GISSI-HF Trial): A Randomised, Double-Blind, Placebo-Controlled Trial. Tavazzi L, Maggioni AP, Marchioli R, et al. Lancet (London, England). 2008;372(9645):1231-9. doi:10.1016/S0140-6736(08)61240-4.
5. Assessment of Adverse Effects Attributed to Statin Therapy in Product Labels: A Meta-Analysis of Double-Blind Randomised Controlled Trials. Cholesterol Treatment Trialists' (CTT) Collaboration. Electronic address: ctt@ndph.ox.ac.uk, Cholesterol Treatment Trialists' (CTT) Collaboration. Lancet (London, England). 2026;407(10529):689-703. doi:10.1016/S0140-6736(25)01578-8.
6. Lowering Cholesterol, Blood Pressure, or Both to Prevent Cardiovascular Events: Results of 8.7 Years of Follow-Up of Heart Outcomes Evaluation Prevention (HOPE)-3 Study Participants. Bosch J, Lonn EM, Jung H, et al. European Heart Journal. 2021;42(31):2995-3007. doi:10.1093/eurheartj/ehab225.
7. Cholesterol Lowering in Intermediate-Risk Persons without Cardiovascular Disease. Yusuf S, Bosch J, Dagenais G, et al. The New England Journal of Medicine. 2016;374(21):2021-31. doi:10.1056/NEJMoa1600176.
8. Crestor. Food and Drug Administration. Updated date: 2026-04-29.
9. Long-Term Mortality After Blood Pressure-Lowering and Lipid-Lowering Treatment in Patients With Hypertension in the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) Legacy Study: 16-Year Follow-Up Results of a Randomised Factorial Trial. Gupta A, Mackay J, Whitehouse A, et al. Lancet (London, England). 2018;392(10153):1127-1137. doi:10.1016/S0140-6736(18)31776-8.
10. Challenging Issues in Clinical Trial Design: Part 4 of a 4-Part Series on Statistics for Clinical Trials. Pocock SJ, Clayton TC, Stone GW. Journal of the American College of Cardiology. 2015;66(25):2886-2898. doi:10.1016/j.jacc.2015.10.051.
11. Cholesterol Lowering, Cardiovascular Diseases, and the Rosuvastatin-JUPITER Controversy: A Critical Reappraisal. de Lorgeril M, Salen P, Abramson J, et al. Archives of Internal Medicine. 2010;170(12):1032-6. doi:10.1001/archinternmed.2010.184.
12. Evaluation of Time to Benefit of Statins for the Primary Prevention of Cardiovascular Events in Adults Aged 50 to 75 Years: A Meta-analysis. Yourman LC, Cenzer IS, Boscardin WJ, et al. JAMA Internal Medicine. 2021;181(2):179-185. doi:10.1001/jamainternmed.2020.6084.
13. Long-Term Efficacy and Safety of Statin Treatment Beyond Six Years: A Meta-Analysis of Randomized Controlled Trials With Extended Follow-Up. Lv HL, Jin DM, Liu M, et al. Pharmacological Research. 2014;81:64-73. doi:10.1016/j.phrs.2014.02.006.
Updates
Get low- and no-cost health tips and root-cause solutions.
FrugalDoc
Affordable Health & Wellness
© 2025 FrugalDoc Health & Wellness. All rights reserved.